- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
Thyroid gland
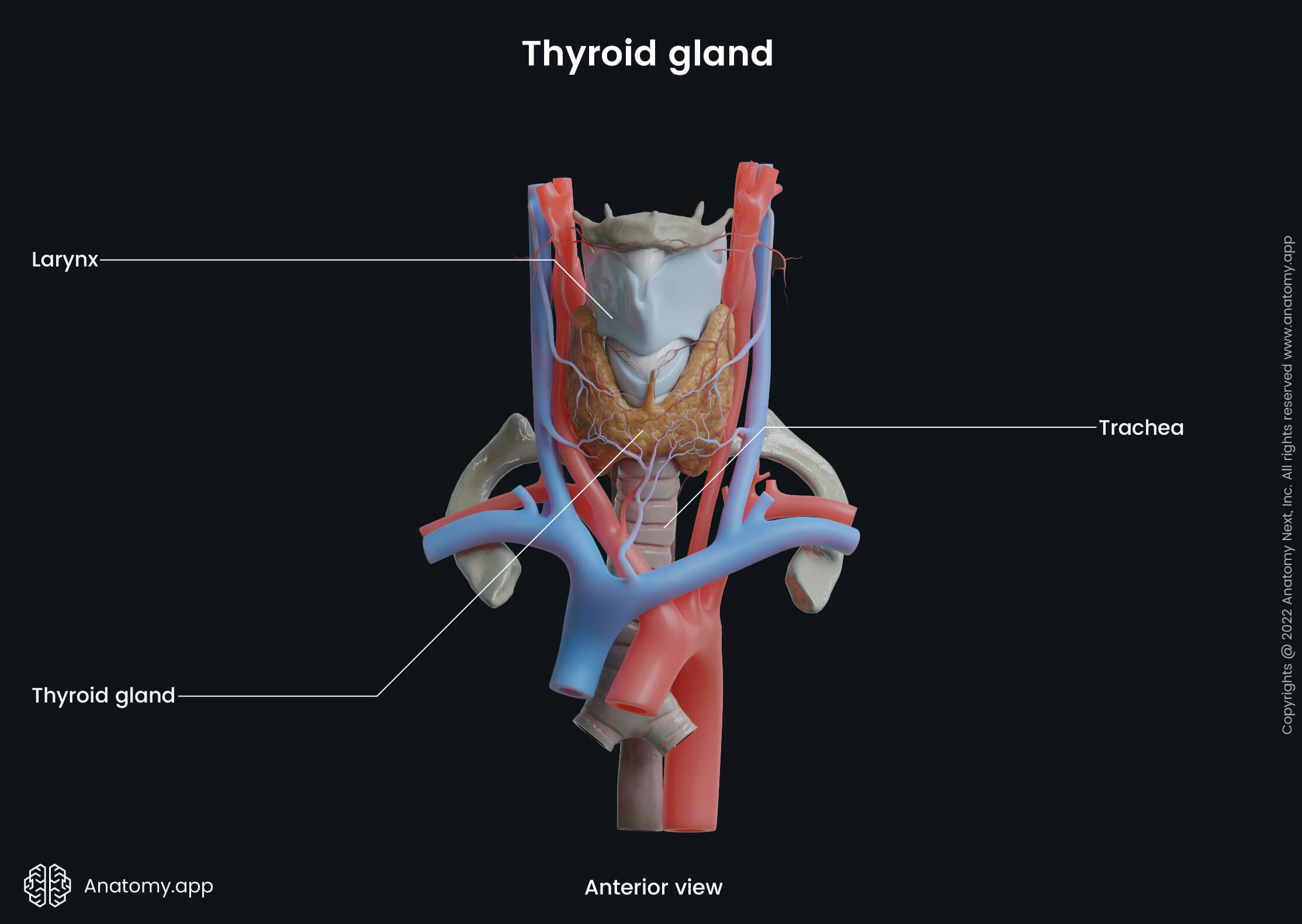
The thyroid gland (or simply the thyroid, Latin: glandula thyreoidea) is an endocrine organ located in the anterior neck region. It lies below the thyroid cartilage, adjacent to the larynx and trachea. The thyroid consists of two lobes connected by an isthmus in the middle. The gland produces hormones thyroxine (T4) and triiodothyronine (T3), which are essential to normal metabolism, growth, and development. It also produces calcitonin, a hormone that is involved in calcium homeostasis.

Thyroid gland location
The thyroid gland is a butterfly-shaped organ located in the midline of the neck over the trachea below the thyroid cartilage. It is situated behind the sternohyoid and sternothyroid strap muscles and between the middle layers of the deep cervical fascia. The normal-sized thyroid extends from the level of the 5th cervical vertebra (C5) to the first thoracic vertebra (T1).
Thyroid gland anatomy
The adult gland typically weighs around 20 g. The thyroid gland of females tends to be larger than in males as it can increase in size and weight during pregnancy and menstruation. The thyroid gland is made up of two lobes (right and left) that are connected by an isthmus in the middle. The lobes make up the majority of the gland's volume. Both lobes are located in the lower aspect of the anterior neck triangles.
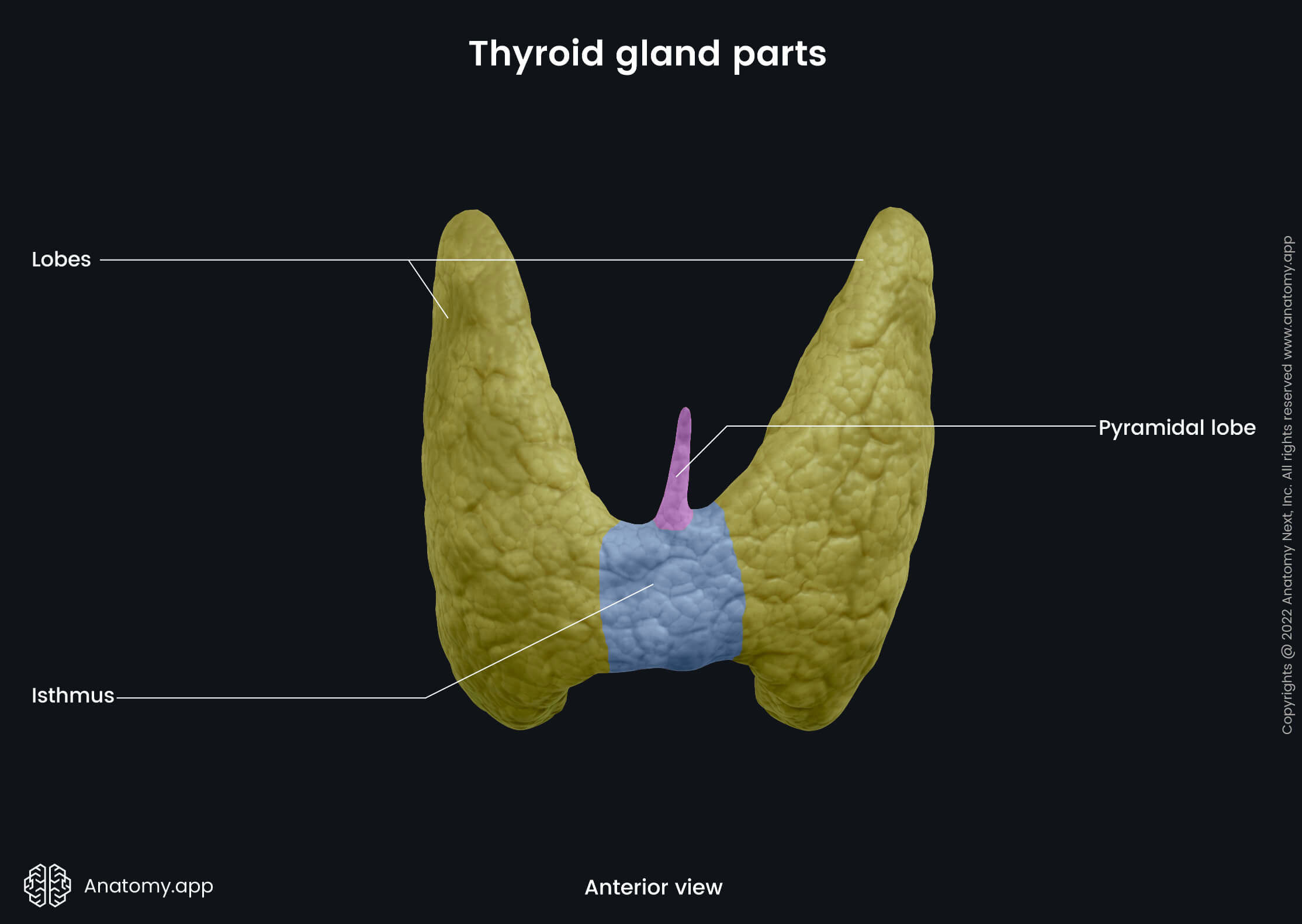
A thyroid lobe normally is conical in shape and approximately 4 to 6 cm in length. Both lobes extend from the oblique line of the thyroid cartilage to the fourth or fifth tracheal cartilages. The size of the isthmus is typically 2 to 3 mm. It can easily be palpated in the midline of the neck inferiorly to the arch of the cricoid. On occasion, the isthmus can be absent.
Some people have an additional pyramidal lobe extending upward from the isthmus as a caudal remnant of the thyroglossal duct. Sometimes ectopic tissue of the thyroid gland in the form of nodules or cysts, or even entirely ectopic thyroid glands can be found anywhere between the isthmus and the base of the tongue.
Thyroid gland surfaces and related structures
The whole thyroid gland is surrounded by the middle or pretracheal layer of the deep cervical fascia. The fascia also forms the suspensory ligament of Berry that fixates the gland to the trachea and larynx (cricoid cartilage). This makes the gland move during swallowing. The thyroid gland is also enveloped by a fibrous capsule. Septae extending from the capsule go into the parenchyma (functional tissue) of the gland and divide it into lobes and lobules.
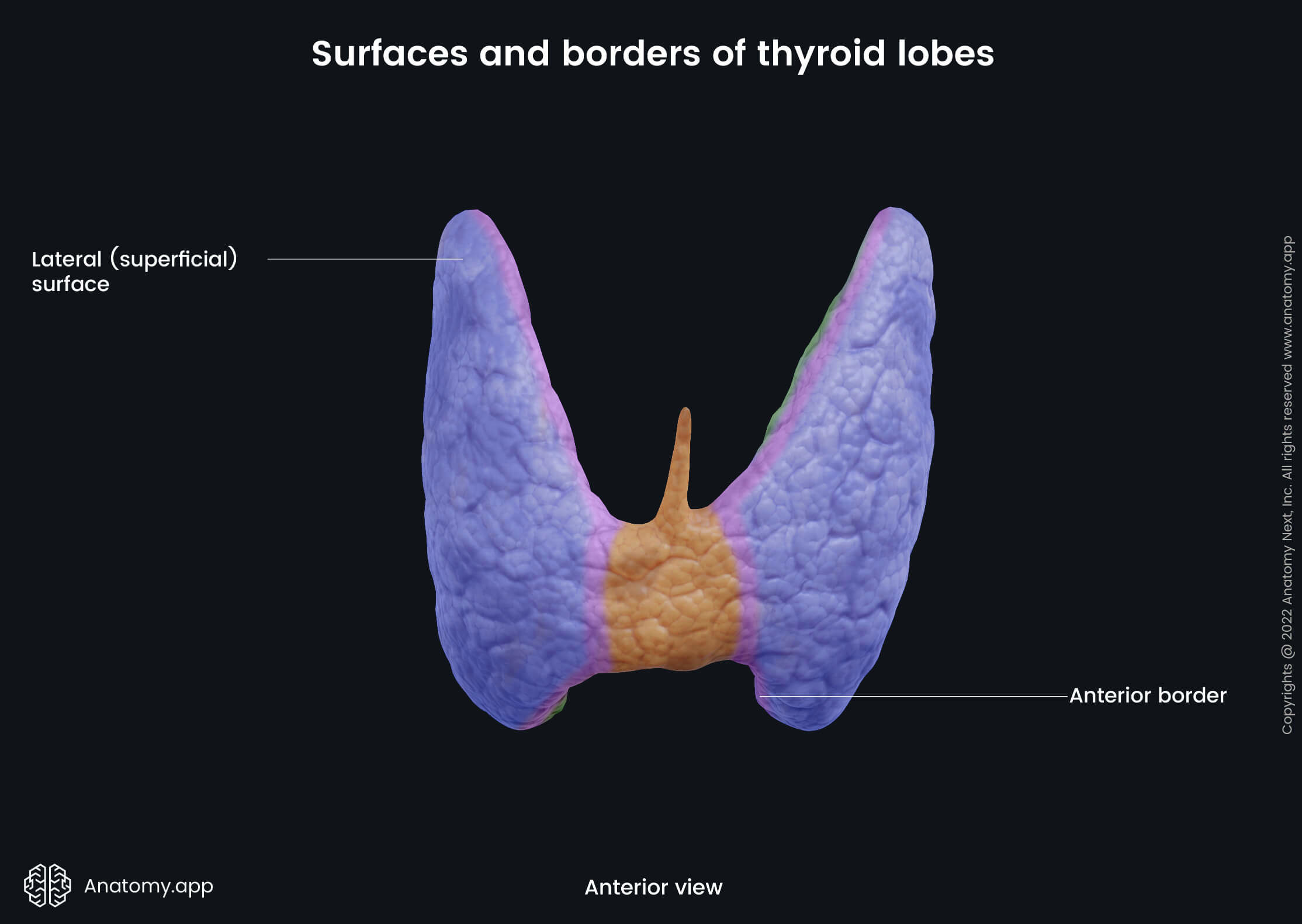
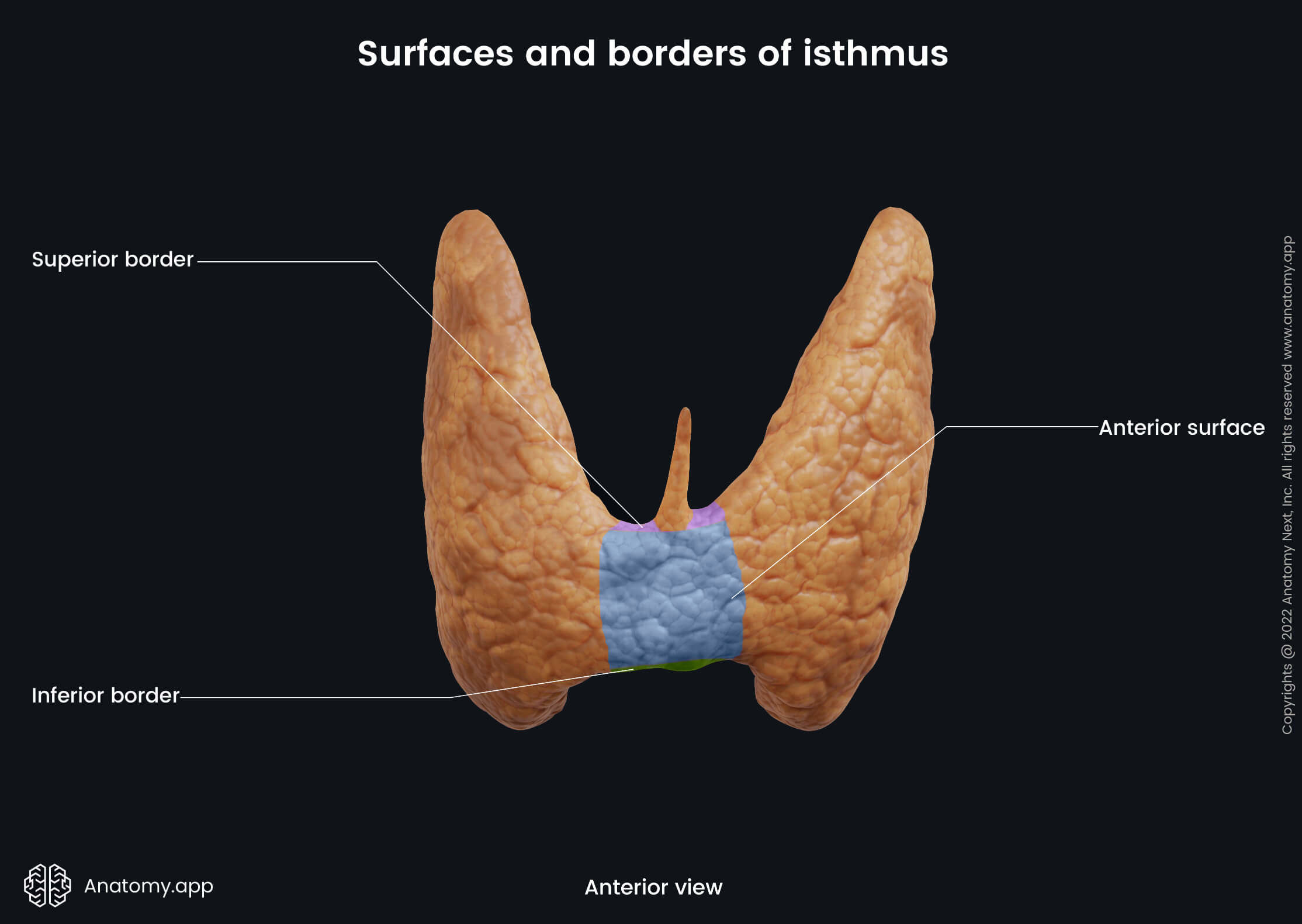
Each thyroid lobe has a base and an apex, three surfaces (lateral or superficial, medial or deep, and posterolateral) and two borders (anterior and posterior). The isthmus of the thyroid has two surfaces (anterior and posterior) and two borders (superior and inferior).
Surfaces and borders of thyroid gland lobes
The lateral (or superficial) surface of the thyroid gland is covered by infrahyoid strap muscles - the sternothyroid, the superior belly of the omohyoid and the sternohyoid more anteriorly. It is also covered by the anterior border of the sternocleidomastoid muscle that lies more inferiorly.
The medial (or deep) surface of the gland lies next to the cricoid and thyroid cartilages of the larynx, trachea, and esophagus. Superior to this surface are located two muscles - the inferior pharyngeal constrictor and the posterior part of the cricothyroid. And posteriorly it is crossed by two nerves - external laryngeal nerve and recurrent laryngeal nerve.
The third surface of the thyroid is known as the posterolateral surface. Next to this surface, the carotid space can be found. This space contains the common carotid artery, internal jugular vein and vagus nerve (CN X).
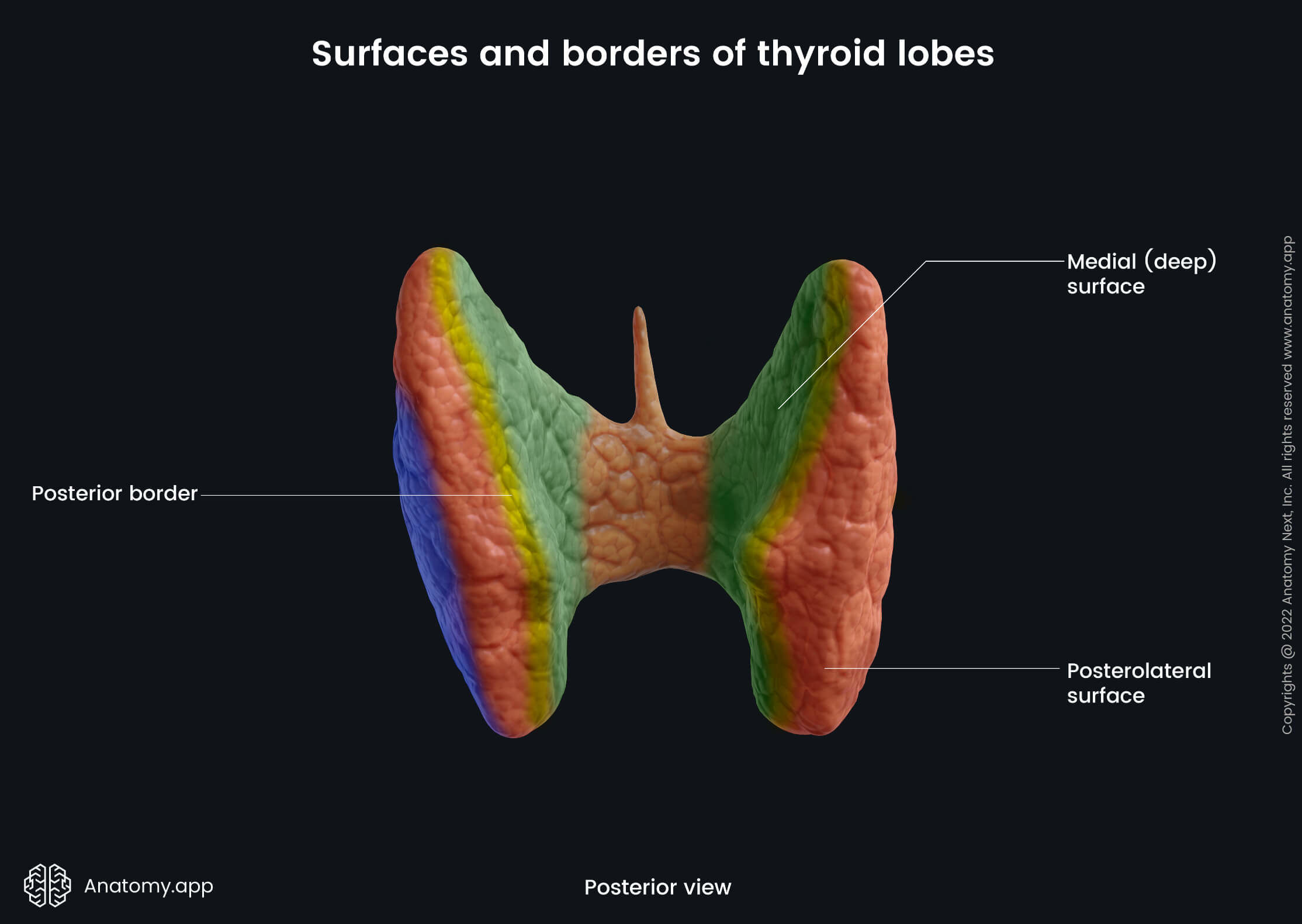
The anterior border of the thyroid is related to the superior thyroid artery. The posterior border separates medial and posterolateral surfaces. This border is related to the inferior thyroid artery and its anastomosis with the superior thyroid artery. The thoracic duct lies near the posterior border of the left lobe. Paratracheal lymph nodes and parathyroid glands are additional important structures related to this border.
Surfaces and borders of isthmus
The anterior surface of the isthmus is covered by the sternothyroid and sternohyoid muscles and it is crossed by the anterior jugular vein. The posterior surface rests on the surfaces of the 2nd and 3rd tracheal cartilages. The superior border of the isthmus relates to the anastomosis of the right and left superior thyroid arteries. And the inferior border is where the inferior thyroid veins leave the gland.

Vascular supply of thyroid gland
Arterial blood supply
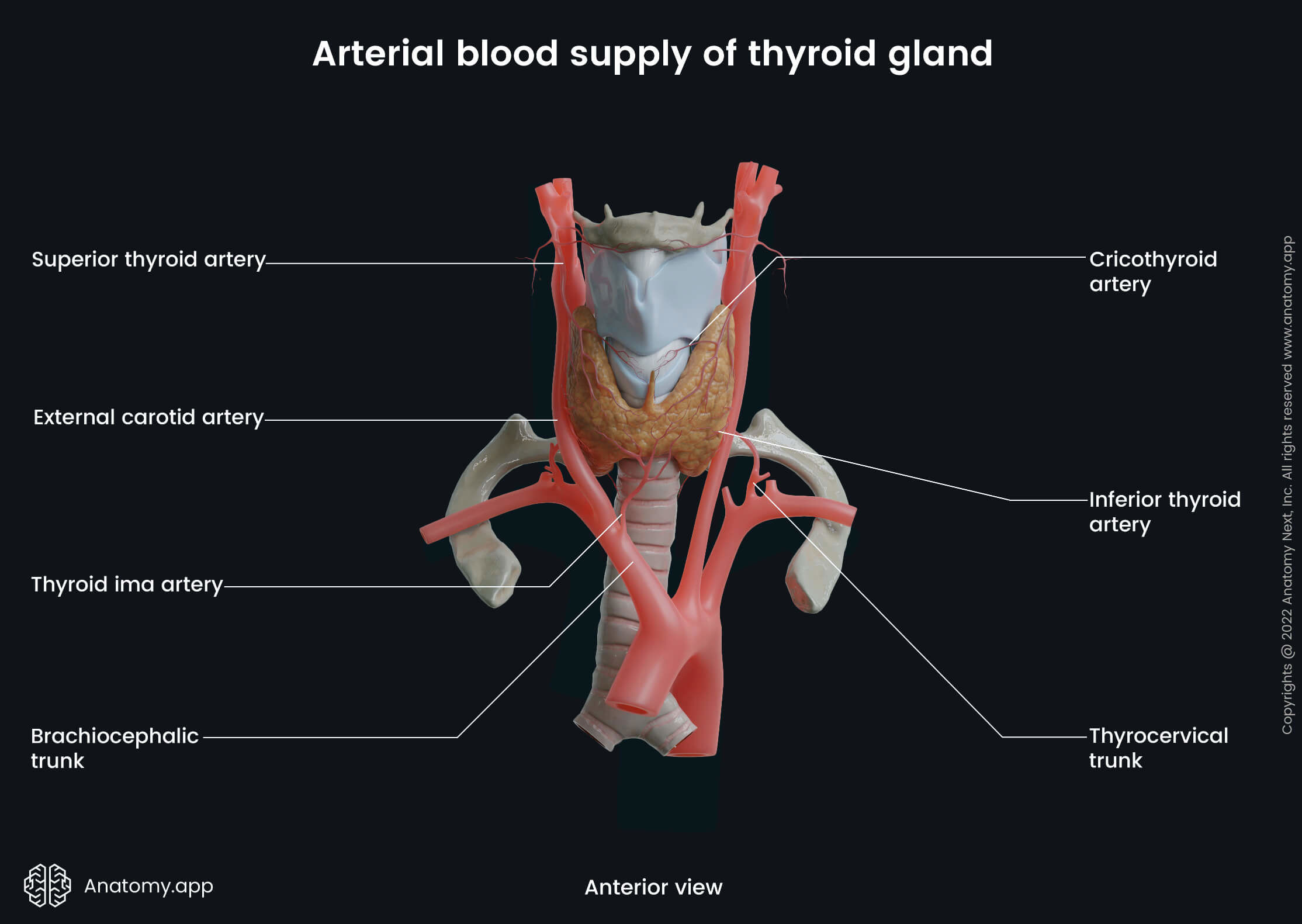
The thyroid gland has a rich blood vessel network. The main arteries that contribute to its blood supply are the superior and inferior thyroid arteries. They are two bilateral pairs that anastomose with each contralateral artery.
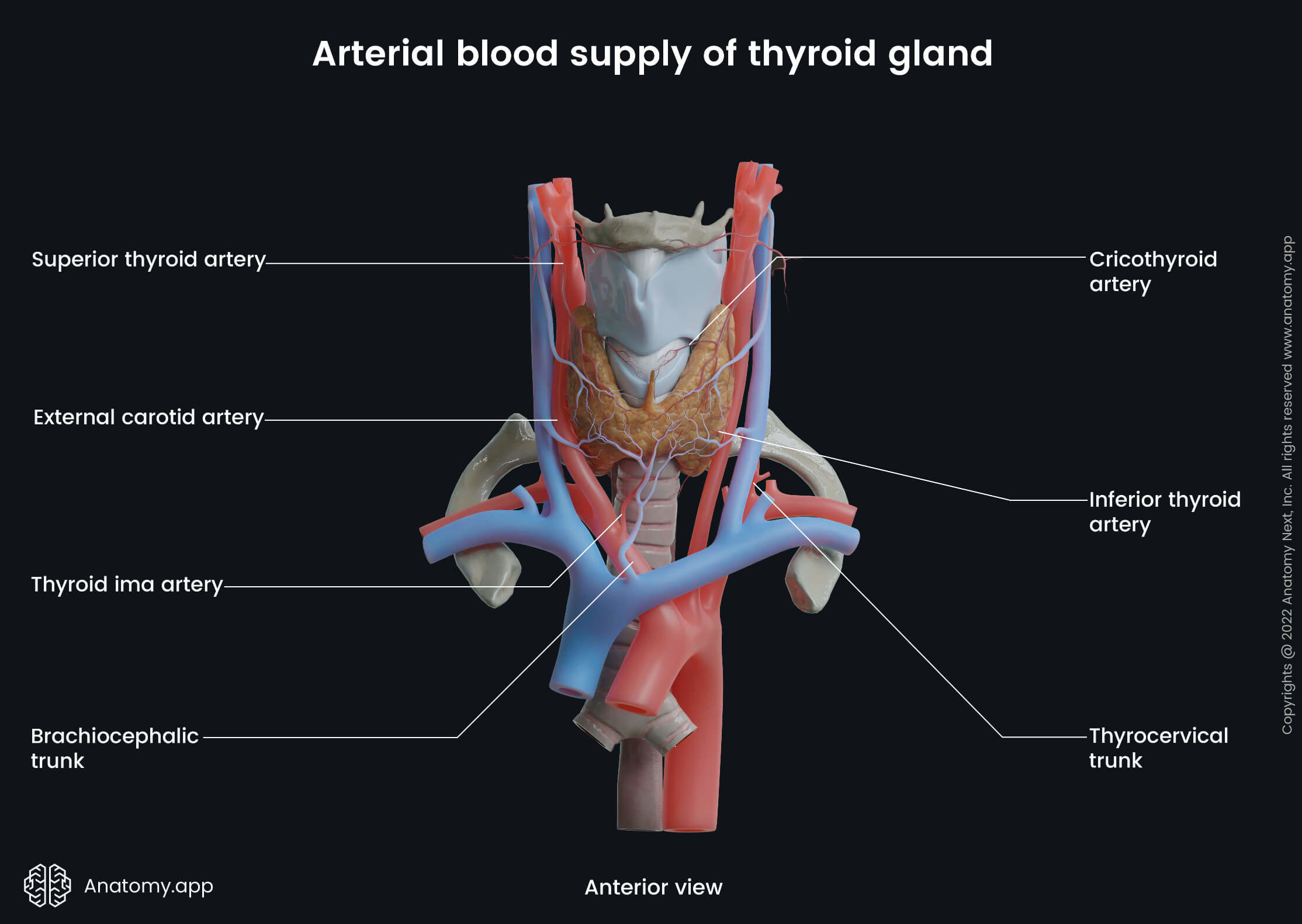
The superior thyroid arteries branch off the external carotid arteries and supply the upper parts of the thyroid lobes. The inferior thyroid arteries, on the other hand, originate from the thyrocervical trunks of the subclavian arteries and supply the inferior and posterior parts of the thyroid.
A very rare additional artery called the thyroid ima artery can be found in some individuals. It usually branches off from the aortic arch or the brachiocephalic trunk and supplies the isthmus or the inferior part of the thyroid gland.
Note: the recurrent laryngeal nerve (RLN), which innervates the larynx, perpendicularly passes the inferior thyroid artery approximately at the point where the artery turns its course to reach the posterolateral surface of the thyroid. The RLN passes either in front of or behind the inferior thyroid artery. The many anatomical variations of both structures are challenging during thyroid gland surgery. One of the major complications of thyroidectomy in case of RLN damage is hoarseness and breathing difficulties.
Venous drainage
The venous drainage occurs through three main pathways – via the superior, middle, and inferior thyroid veins. All mentioned veins emerge from the glandular venous plexus. It is a venous network made of all thyroid veins and located on the surfaces of the thyroid gland.
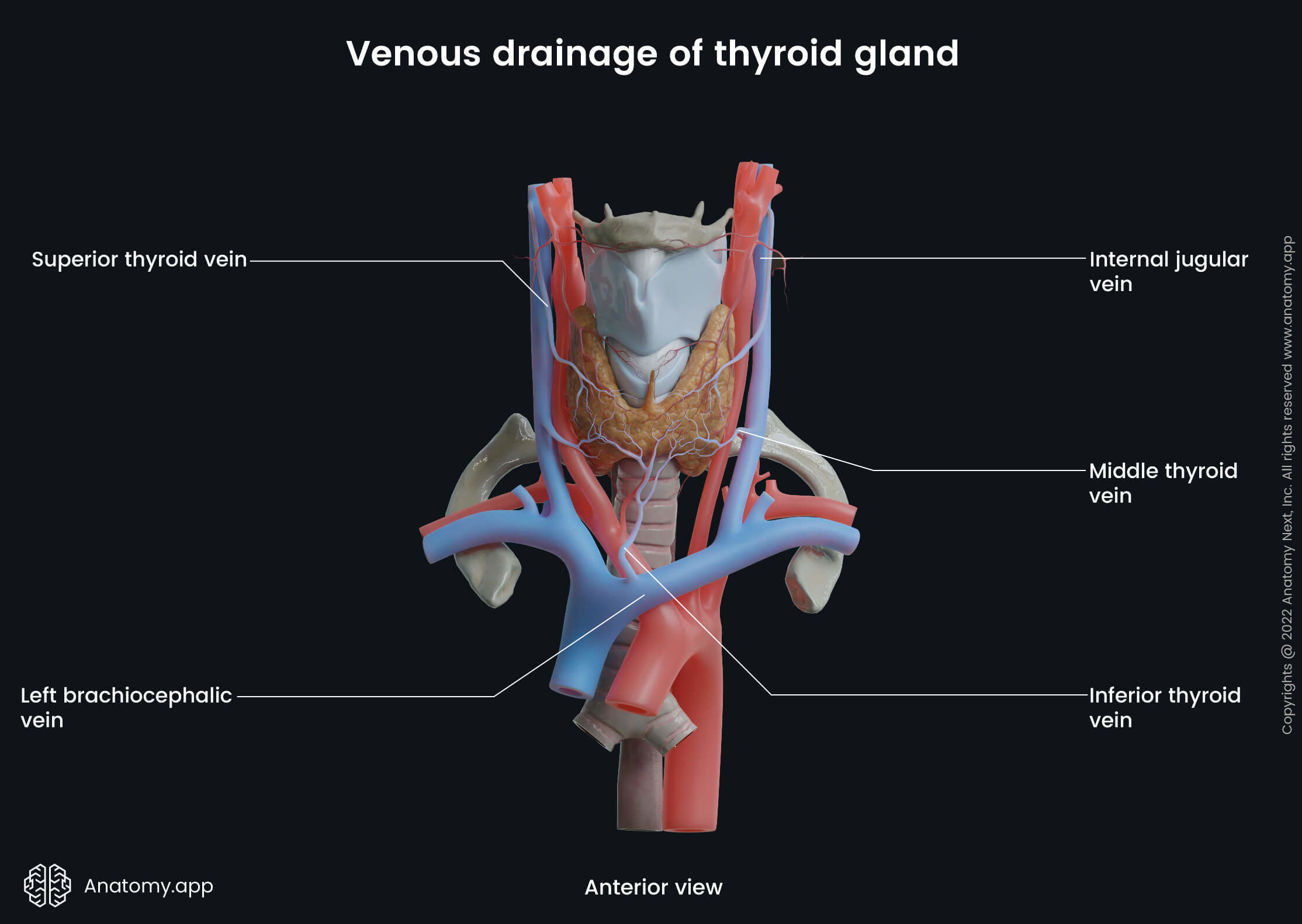
The superior thyroid veins collect blood from the upper part of the thyroid and drain into the internal jugular veins. The superior thyroid vein communicates with the superior laryngeal vein and cricothyroid vein, additionally draining blood from the larynx as well. The middle thyroid veins originate from the inferolateral part of the gland and also drain into the internal jugular vein.
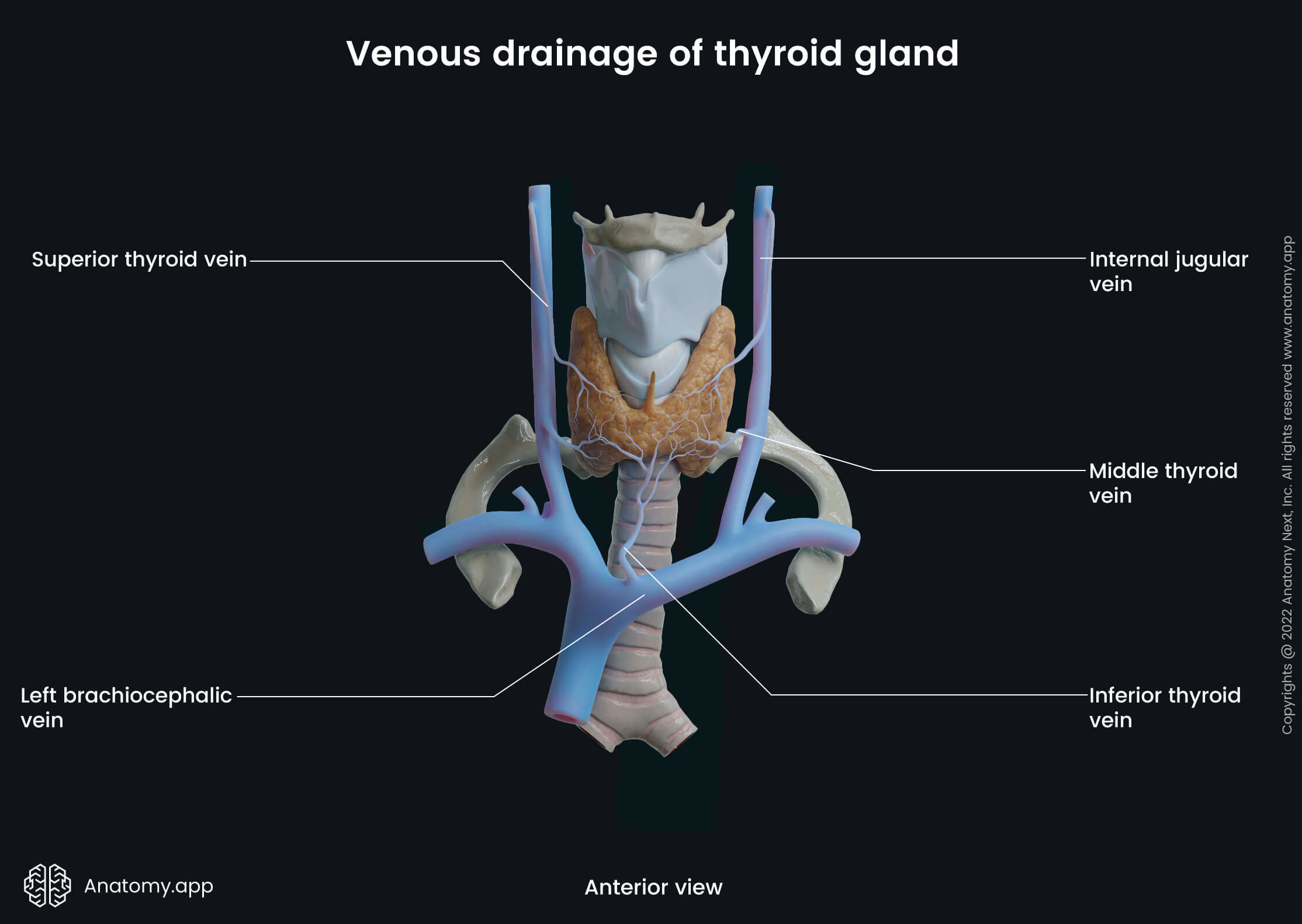
A pair of inferior thyroid veins drains venous blood from the lower parts of the gland. They also communicate with esophageal, tracheal, and inferior laryngeal veins. The inferior thyroid vein on the left side joins the left brachiocephalic vein. The right inferior thyroid vein, however, travels across the right brachiocephalic artery, joining the right brachiocephalic vein close to its junction site with the superior vena cava. Sometimes the inferior thyroid veins can also flow directly into the superior vena cava or the left brachiocephalic vein via one common trunk.
Lymphatic drainage
Anatomical structures that provide lymphatic drainage of the thyroid gland are connected with other nearby lymphatic system structures of the neck via a network of lymph vessels. The first and the closest lymph nodes in this lymphatic network are the perithyroidal lymph nodes which are positioned between both of the carotid arteries, hyoid bone, and sternal notch. Lymphatic vessels extend all the way to the lymph nodes in the posterior triangle of the neck, as well as to the lateral part where jugular lymph nodes are located. Additionally, lower deep cervical, prelaryngeal, pretracheal, paratracheal and superior mediastinal lymph nodes contribute to the lesser part of the lymphatic drainage.
Innervation of thyroid gland
The autonomic nervous system provides innervation to the thyroid gland. Through cervical sympathetic ganglia and parasympathetic fibers of the vagus nerve, it contributes to the nerve network of the thyroid.
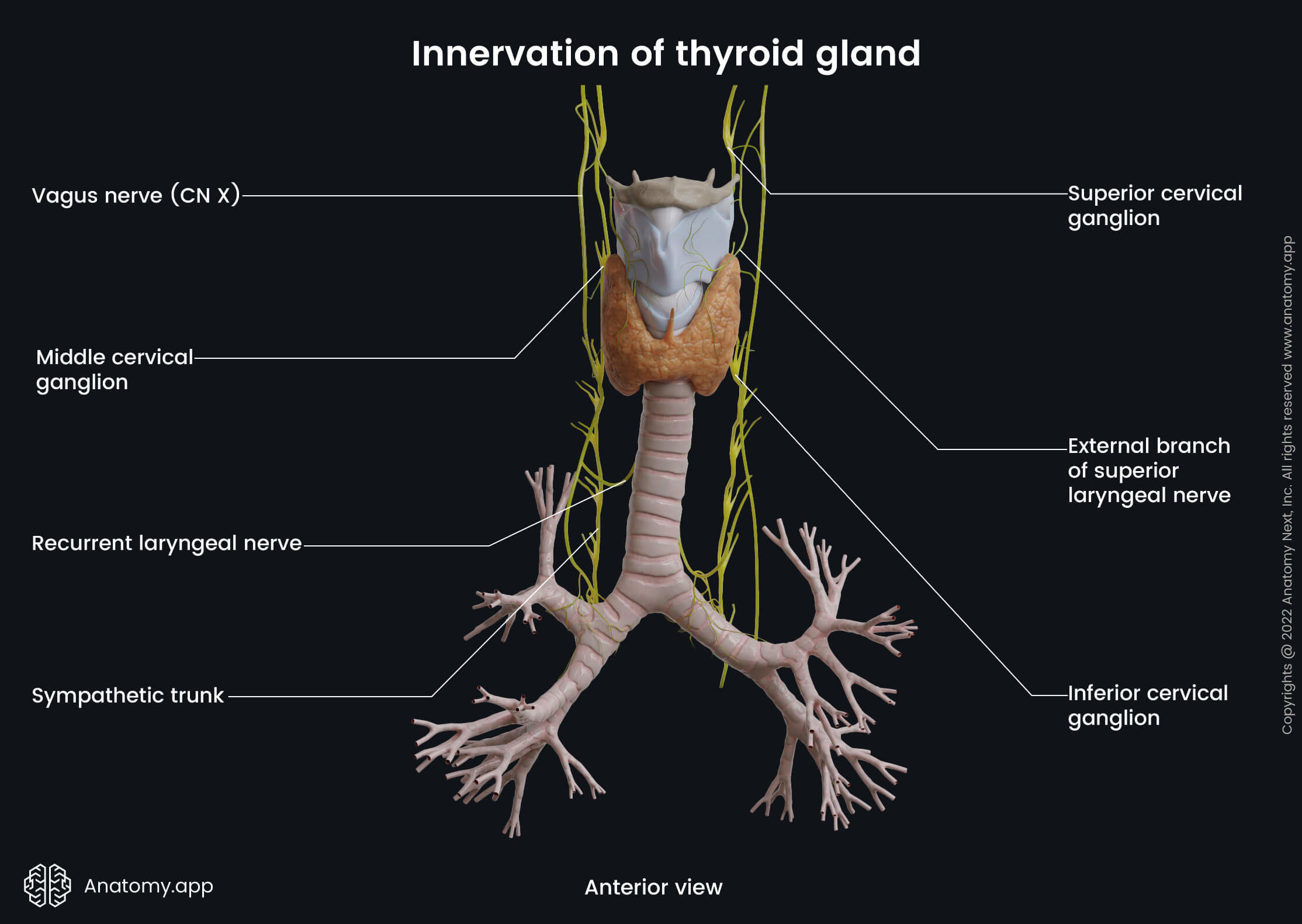
The cervical sympathetic ganglia contain three subdivisions - superior, middle, and inferior cervical ganglia - directly providing innervation from the sympathetic trunk. The fibers of the inferior ganglion create a plexus around the inferior thyroid artery. This plexus also communicates with the recurrent laryngeal nerve, external branch of the superior laryngeal nerve, superior cardiac nerve fibers, and the fibers of the common carotid artery plexus.
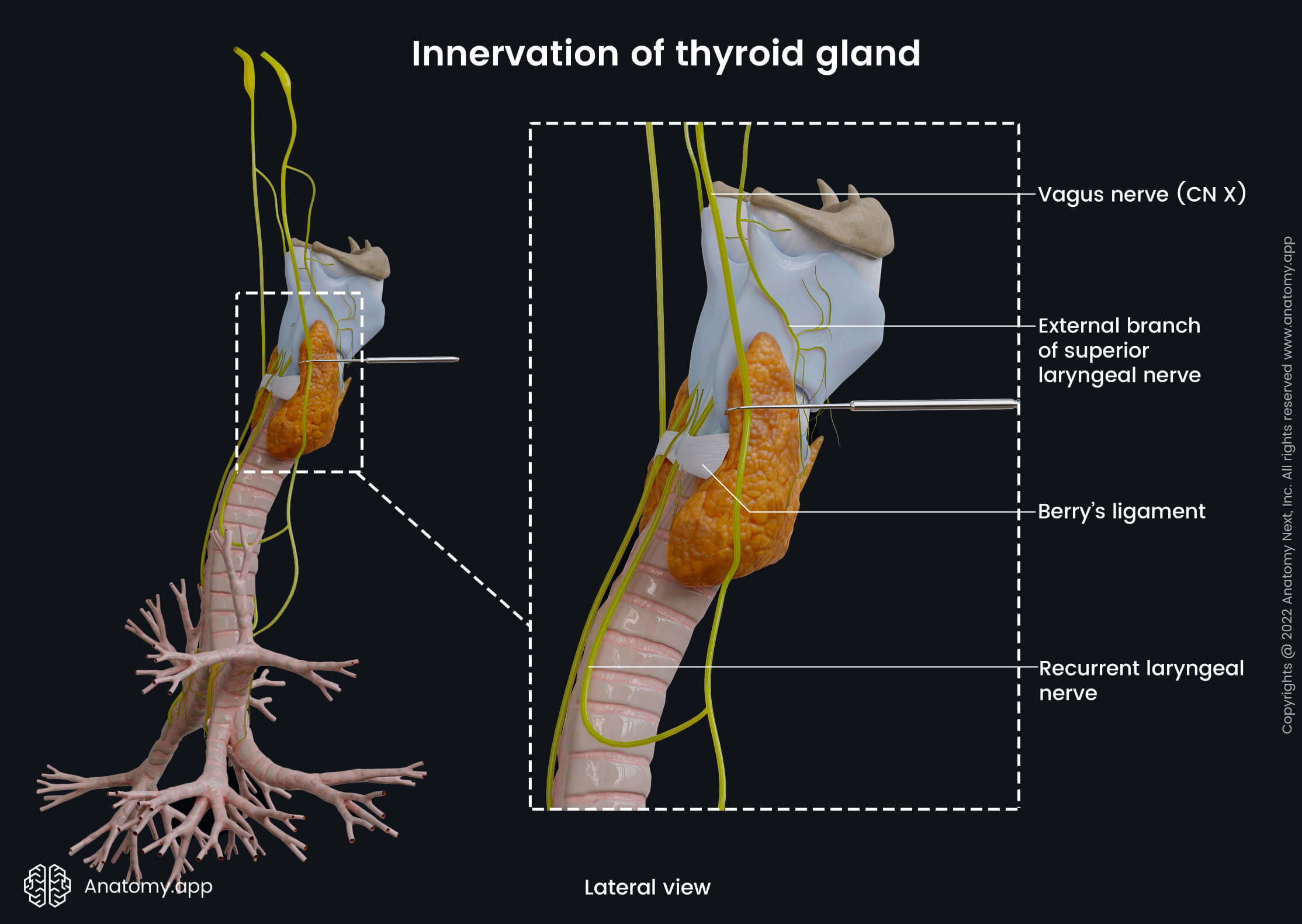
The parasympathetic nerve fibers that innervate the thyroid mainly arise from the superior laryngeal nerve and the recurrent laryngeal nerve. Both mentioned nerves are branches of the tenth cranial nerve - the vagus nerve (CN X).
Thyroid gland histology
The thyroid gland is composed of multiple spherical-shaped structures called follicles. A thyroid follicle is a functional and structural unit of the thyroid gland. A single layer of thyroid follicular cells surrounds the interior of the follicle, which is filled with a gel-like fluid called colloid. The colloid consists of a protein named thyroglobulin, which is a precursor to active thyroid hormones - triiodothyronine (T3) and tetraiodothyronine or thyroxine (T4). The space between the follicles (termed interstitium) is surrounded by connective tissue and is rich in the capillary, nervous and lymphatic network.
There are two main types of cells found in the parenchyma of the thyroid gland:
- Follicular cells (or thyrocytes) - thyroid epithelial cells that produce and secrete the thyroid hormones (T3 and T4). The activity of the follicular cells is controlled by a thyroid-stimulating hormone (TSH, thyrotropin) that is produced by the anterior pituitary (also known as hypophysis).
- Parafollicular cells (also called C cells) - these cells secrete a hormone called calcitonin that is responsible for regulating the calcium level in the blood. They are located mainly between the follicular epithelial cells or in the thyroid interstitium within the wall of the thyroid follicles. C cells are found primarily in the middle and superior parts of the thyroid lobes.
Thyroid gland function
Production and secretion of hormones (thyroid hormones T4 and T3, and calcitonin) is the main function of the thyroid gland. In general, the thyroid hormones are crucial for normal function and regulation of all organ systems and body metabolism, as well as maintaining calcium blood equilibrium.
Thyroid hormone synthesis and its regulation
The thyroid hormone synthesis happens within the thyroid follicle. The whole process is complex and requires iodine. Iodine is absorbed in the stomach and small intestine during dietary intake and then distributed in the extracellular space from the bloodstream. After reaching the follicular cell, iodine begins a cascade of various complex reactions and processes. Through the joining of several iodine molecules, tetraiodothyronine or thyroxine (T4) and triiodothyronine (T3) are formed.
These thyroid hormones are then stored in the colloid and released after stimulation of the thyroid-stimulating hormone (TSH). With the help of transport proteins, hormones can reach their target tissue. T3 is a more potent form than T4 because it has a less strong bond with transport proteins. Therefore, it can act and bind with the nuclear receptors more rapidly.
Thyroid hormone production is regulated by the so-called hypothalamic - pituitary - thyroid axis. It is an autoregulatory feedback mechanism. When T4 and T3 levels in blood serum are detected as low, this triggers the hypothalamus. The hypothalamus then induces the anterior pituitary to produce TSH by releasing the thyrotropin-releasing hormone (TRH) that stimulates the production of the TSH. Similarly, if the thyroid hormone levels in the blood are high, structures of the axis decrease the production of TSH.
Iodine
Iodine has a vital role in thyroid hormone synthesis. Therefore adequate iodine dietary intake is crucial. The average necessary intake should be at least 0,1 mg of iodine daily. Iodination of salt has largely prevented dietary iodine deficiency, mainly in developed countries. However, it still remains a significant public health problem worldwide, especially in younger children and pregnant women.
Iodine deficiency is associated with an increased death rate during birth and mental retardation (also called endemic cretinism) because of the brain damage caused by the lack of iodine. But this condition is potentially preventable. Endemic goiter is a form of thyroid enlargement due to dietary iodine deficiency and subsequent TSH overproduction. Endemic goiter is particularly common in countries where the soil is low in iodine due to glaciation or especially in mountain regions. These aforementioned iodine-deficiency disorders (IDDs) are considered the most common endocrine disorders in the world. Nevertheless, they are the most preventable as well.
Effects of thyroid hormones
Thyroid hormones have many physiological effects on the target tissues. They are essential for metabolism, growth and development of the organism. On the cellular level, they control the gene expression of enzymes necessary for cell functioning.
For example, in the myocardium, T3 promotes the expression of heart muscle cell chains and the metabolic enzyme called adenosine triphosphatase (ATPase). It leads to increased strength of muscle cell contractions and stimulation of systolic myocardial contraction and diastolic myocardial relaxation. T3 also increases the heart rate by affecting repolarization and depolarization in the sinoatrial node of the heart.
In the liver, on the other hand, T3 increases the expression of low-density lipoprotein (LDL) cholesterol receptors and influences LDL cholesterol metabolism. Thyroid hormones also boost cellular metabolic activity by increasing the number and size of cell mitochondria and their enzyme activity. It all leads to an increase in cellular oxygen consumption, glucose metabolism and ATP production.
These hormones also affect gastric motility, respiration and bone metabolism. They are responsible for mental alertness, enhancing memory and focus. In pregnancy, thyroid hormones are crucial for fetal growth and development, especially the central nervous system development.
Calcitonin
The parafollicular cells of the thyroid (C cells) are responsible for production of a hormone called calcitonin. The main goal of calcitonin is to maintain calcium blood homeostasis (maintaining normal calcium levels in blood) through the increase of osteoblast activity and suppression of osteoclast activity in bones, decrease in calcium absorption in the gastrointestinal tract and increase in the urinary calcium excretion in the kidneys. This, in turn, leads to a decrease of calcium concentration in the serum.
Thyroid gland diseases
The most common thyroid disorders include abnormalities in thyroid hormone production (hypothyroidism, hyperthyroidism), thyroid nodules and thyroid cancer. Decreased production of thyroid hormones is known as hypothyroidism, while increased hormone production - hyperthyroidism. Hypothyroidism due to dietary iodine deficiency (also called endemic goiter) is the most common endocrine pathology worldwide.
Hypothyroidism
Hypothyroidism is a group of thyroid gland disorders characterized by low production and secretion of thyroid hormones. Hypothyroidism can be primary and secondary. Primary hypothyroidism involves the thyroid gland tissue and manifests as a malfunction or destruction of the thyroid gland itself. Secondary hypothyroidism, on the other hand, is due to dysfunction of the hypothalamus or the pituitary gland.
The most common cause of the underactive thyroid is iodine deficiency, also called endemic goiter. Endemic goiter is encountered primarily in developing countries because of the poor iodine dietary intake.
Other disturbances, mainly in the developed countries, that contribute to hypothyroidism are Hashimoto's thyroiditis (autoimmune-mediated destruction of the gland tissue), surgical removal of the thyroid gland (partial or total thyroidectomy) and dysfunction of thyroid metabolism due to drugs, to name a few.
The most common symptoms seen in people with hypothyroidism include:
- Slow heart rate (bradycardia)
- Lack of energy, fatigue, sleepiness
- Depression
- Slowness in movements, speech and thoughts
- Dry skin, hair loss
- Intolerance to cold weather
- Weight gain and puffy face
Hyperthyroidism
Hyperthyroidism is a condition included in a broader spectrum of disorders called thyrotoxicosis that is characterized by excessive levels of thyroid hormones in the body. Thyrotoxicosis is a clinical state that can manifest due to thyroid gland issues or other conditions, for example, caused by usage of thyroid hormone medication.
Hyperthyroidism, on the other hand, is a term used to describe excessive thyroid hormone production or secretion by the thyroid gland. The most common cause of hyperthyroidism is Graves' disease. It is an autoimmune disorder characterized by the formation of antibodies against TSH receptors. These antibodies bind to the TSH receptors and stimulate the production of thyroid hormones.
Other disorders associated with hyperthyroidism include such conditions as multinodular goiter and TSH-secreting pituitary adenoma (benign tumor in the pituitary gland).
Symptoms of hyperthyroidism are mainly opposite to hypothyroidism:
- Rapid heart rate (tachycardia) and palpitations
- Nervousness, anxiety, mood swings
- Tremor, muscle weakness
- Heat intolerance, excessive sweating
- Weight loss and increased appetite
- Bulging eyes
Thyroid nodules
A thyroid nodule is a cystic or solid thickening of the thyroid gland tissue that can either be seen or felt during palpation. Thyroid nodules are relatively common, mostly asymptomatic and generally benign. They do not require any particular treatment unless there is a concern for malignancy, signs and symptoms of tissue local compression or hyperthyroidism.
Thyroid cancer
There are various types of thyroid gland cancers depending on the cells they originate from. The most common types are papillary and follicular thyroid carcinomas. According to the classification of the World Health Organization, both types are also known as differentiated thyroid carcinomas as they contain well-developed cells. Both carcinomas arise from the thyroid follicular epithelial cells found in the parenchyma. Papillary thyroid carcinoma constitutes around 90% of all cases. Follicular thyroid carcinoma represents up to 9% of the cases. Both differentiated thyroid carcinomas have the best five-year survival rates.
Medullary thyroid carcinoma is a relatively rare type of cancer. It represents up to 2% of cases (some sources claim it could be up to 10%). This carcinoma originates from the parafollicular C cells. In most cases, it is due to sporadic mutation (meaning, it is not inherited from parents but acquired during lifetime), but in 25% it can be hereditary. Generally, the prognosis is good, especially if diagnosed at an early stage. Nevertheless, despite treatment, it is recurrent in half of the cases.
The most aggressive and the rarest of all thyroid cancers is anaplastic thyroid cancer. It comprises around 1-2% of all cases and has a follicular cell origin. The disease progresses rapidly. Nearly 100% of patients die within six months after the diagnosis is made and even after the treatment has started.
References:
- Brennan, P. P., Standring, S., & Wiseman, S. (2020a). Gray’s Surgical Anatomy (1st ed.). Elsevier.
- Coley, B. D. (2018). Caffey’s Pediatric Diagnostic Imaging, 2-Volume Set (13th ed.). Elsevier.
- Drake, R. L., Vogl, A. W., & Mitchell, A. W. M. (2019). Gray’s Anatomy for Students: With Student Consult Online Access (4th ed.). Elsevier.
- Goldman, L., & Schafer, A. I. (2019). Goldman-Cecil Medicine, 2-Volume Set (Cecil Textbook of Medicine) (26th ed.). Elsevier.
- Hall, J. E., & Hall, M. E. (2021). Pocket Companion to Guyton and Hall Textbook of Medical Physiology. Elsevier.
- Melmed, S., Auchus, R.J., Koenig, R. (2019). Williams Textbook of Endocrinology (14th ed.). Elsevier.
- Standring, S. (2020). Gray’s Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier.
- Townsend, C. M., Jr MD, Beauchamp, R. D., Evers, B. M., & Mattox, K. L. (2021). Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice (21st ed.). Elsevier.
- World Health Organization (2004). Iodine Status Worldwide. WHO Global Database on Iodine Deficiency. Department of Nutrition for Health and Development. Geneva.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app