- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
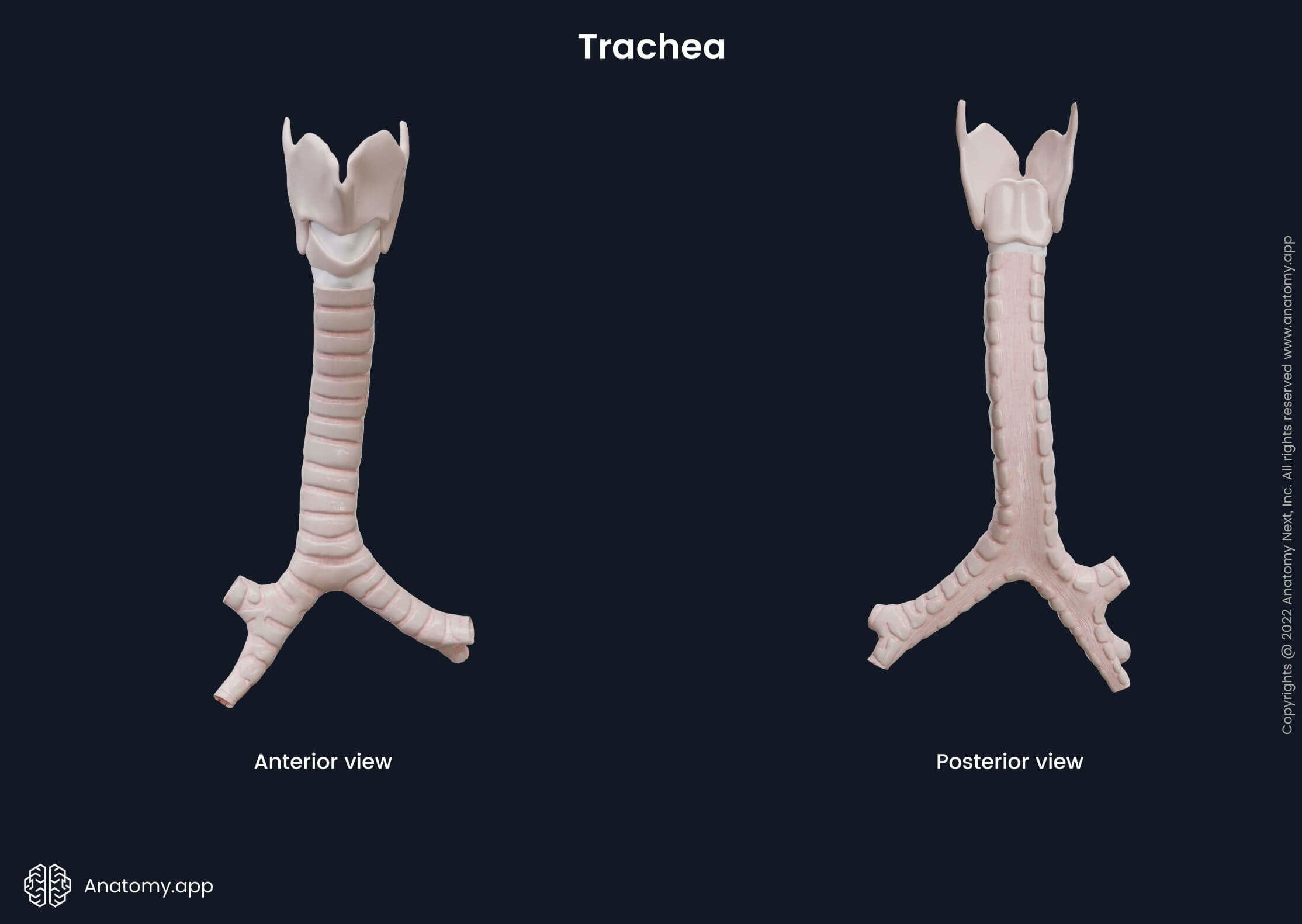
Trachea
The trachea (also known as windpipe, Latin: trachea) is a flexible air tube located in the midline of the neck and rib cage. It is a part of the lower respiratory tract and connects the larynx to the lungs through the bronchial tree.
In adults, the diameter of the trachea is about 0.6 - 1 inches (1.5 - 2.5 cm), and it is around 4 - 5 inches (10 - 13 cm) long. Its size differs in men and women, as the trachea in males is typically wider and longer. The main function of the trachea is to provide the passage of air to and from the lungs. Additionally, it moistens and warms up the passing air, as well as participates in the coughing reflex.
Gross anatomy of trachea
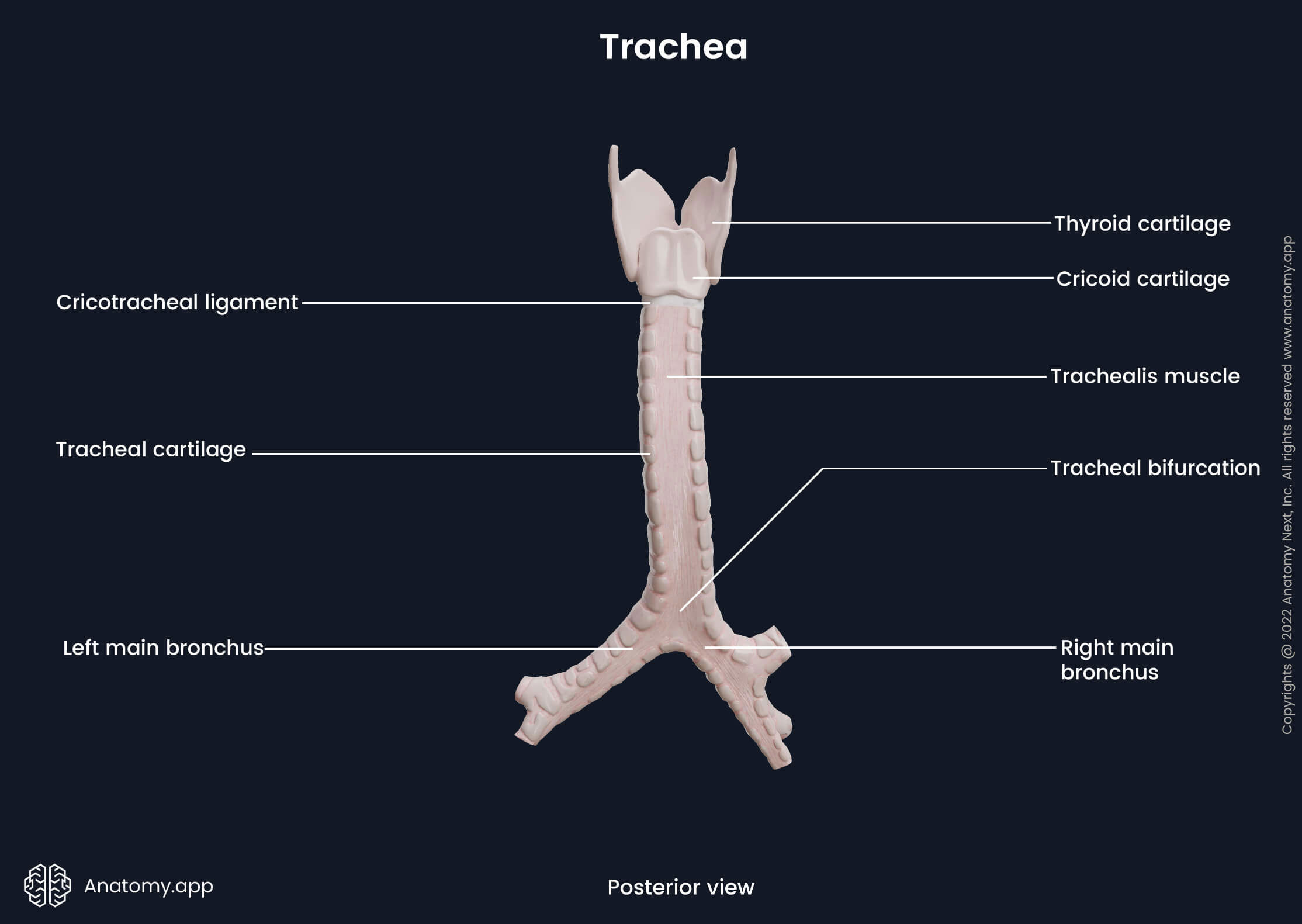
The trachea is composed of fifteen to twenty C-shaped hyaline tracheal cartilages. The posterior part of each ring is made of smooth muscle fibers and connective tissue, forming a fibromuscular membrane known as the trachealis muscle. The tracheal cartilages form the anterolateral wall of the trachea, while the trachealis muscle forms the posterior wall. The trachealis muscle allows the trachea to change its diameter mainly during swallowing when the food bolus (chewed food that is mixed with saliva) goes through the esophagus located posterior to the trachea.
The trachea begins below the cricoid cartilage of the larynx. The mentioned laryngeal cartilage is connected to the first tracheal cartilage by a fibrous structure called the cricotracheal ligament. Each two adjacent tracheal cartilages are joined by circular bands of fibrous connective tissue known as the annular ligaments.
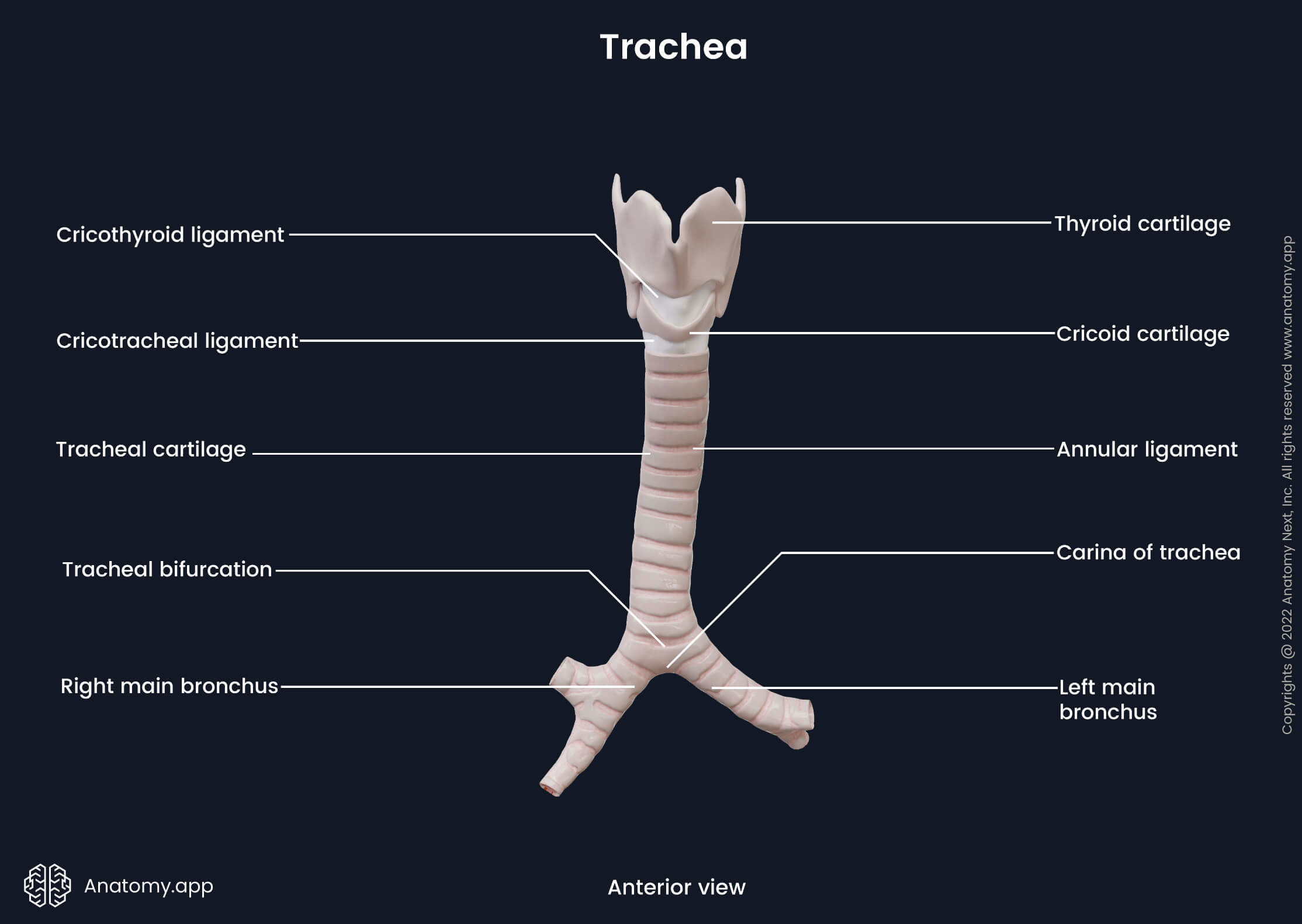
The trachea has two parts: cervical and thoracic. The cervical part extends below the larynx as its continuation, starting from the lower border of the cricoid cartilage at the level of the sixth (in females) or seventh (in males) cervical vertebra (C6 - C7). The thoracic part of the trachea begins at the level of the jugular notch as the trachea enters the rib cage through the superior thoracic aperture. Further, it passes behind the sternum and ends at the cartilaginous ridge called carina. The carina of the trachea serves as a distributor of inhaled airflow between both main bronchi. It projects at the level of the fifth thoracic vertebra (T5), in the middle of the thorax. At this point, the trachea bifurcates and divides into the right and left main bronchi. The bifurcation site is called the tracheal bifurcation.
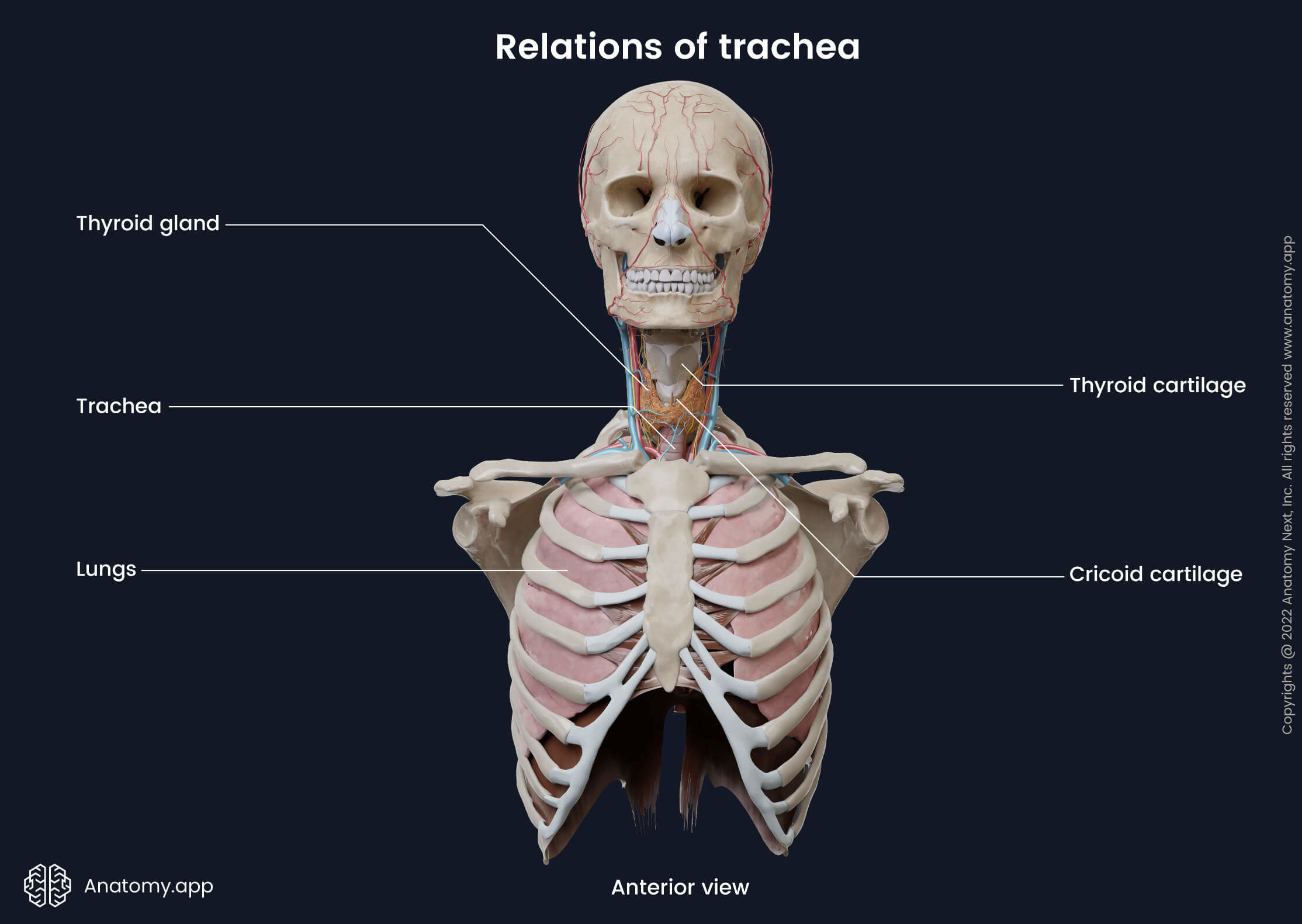
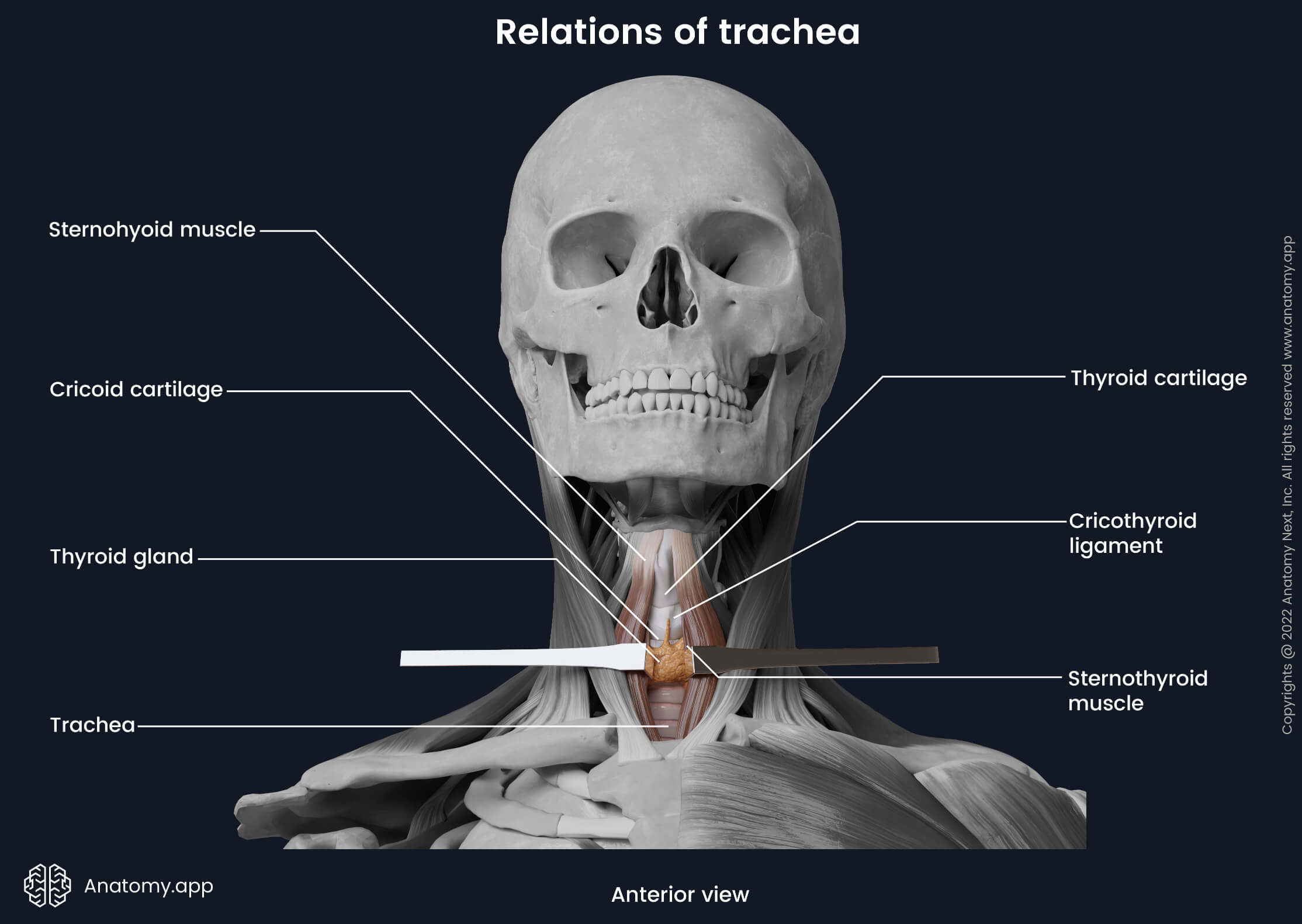
Relations of trachea
Cervical part
Various structures cover the cervical part of the trachea anteriorly. The isthmus of the thyroid gland covers the second to fourth upper tracheal rings. An anastomosis between both superior thyroid arteries lies on the surface of the isthmus at its upper border. Below the isthmus lie the inferior thyroid vein, thyroid ima artery and pretracheal fascia.
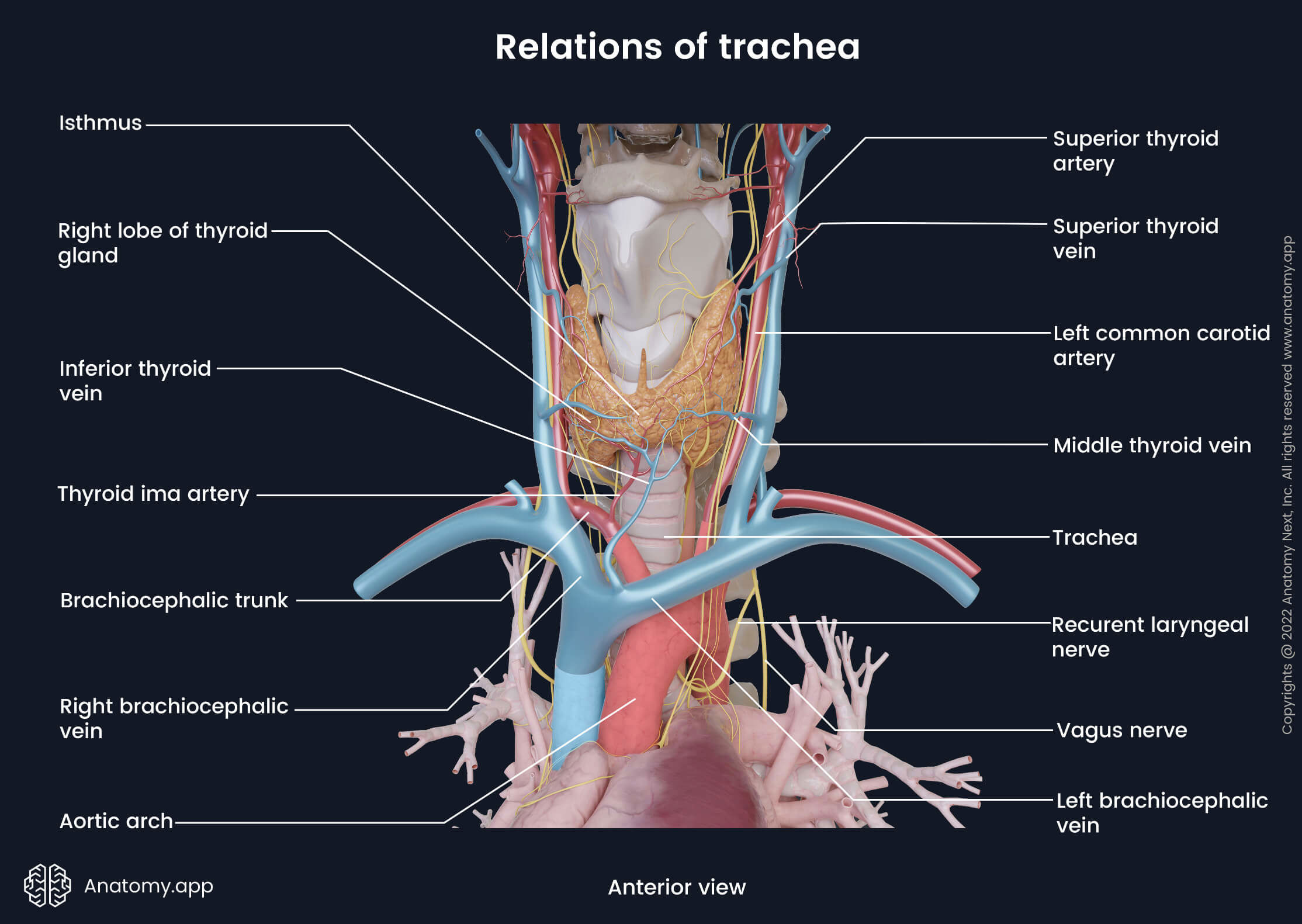
The mentioned structures are covered by the jugular venous arch and infrahyoid muscles of the neck (sternohyoid and sternothyroid). The most superficial layers covering the cervical part of the trachea consist of the superficial cervical fascia and investing layer of the deep cervical fascia, suprasternal space, and finally, skin.
The esophagus lies posteriorly to the trachea, separating it from the spine and prevertebral fascia. The right and left lobes of the thyroid gland reach the level of the fifth and sixth tracheal cartilages laterally. Additionally, the common carotid artery and inferior thyroid arteries lie next to the trachea on each side.
The thyroid gland is enveloped by the pretrachial layer of the deep cervical fascia. This enclosement is known as the false capsule of the thyroid gland. It forms the so-called suspensory ligament of the thyroid gland known as Berry's ligament. This ligament attaches the thyroid gland to the trachea and allows the thyroid to move during swallowing. Another essential structure laterally to the trachea is the recurrent laryngeal nerve (a branch of the vagus nerve, CN X), located in the trachea-oesophageal groove.
Clinical note: The suspensory ligament of Berry and inferior thyroid arteries are significant landmarks surgeons use to identify the recurrent laryngeal nerve. During surgical manipulations, damage to the nerve can result in hoarseness and breathing difficulties.
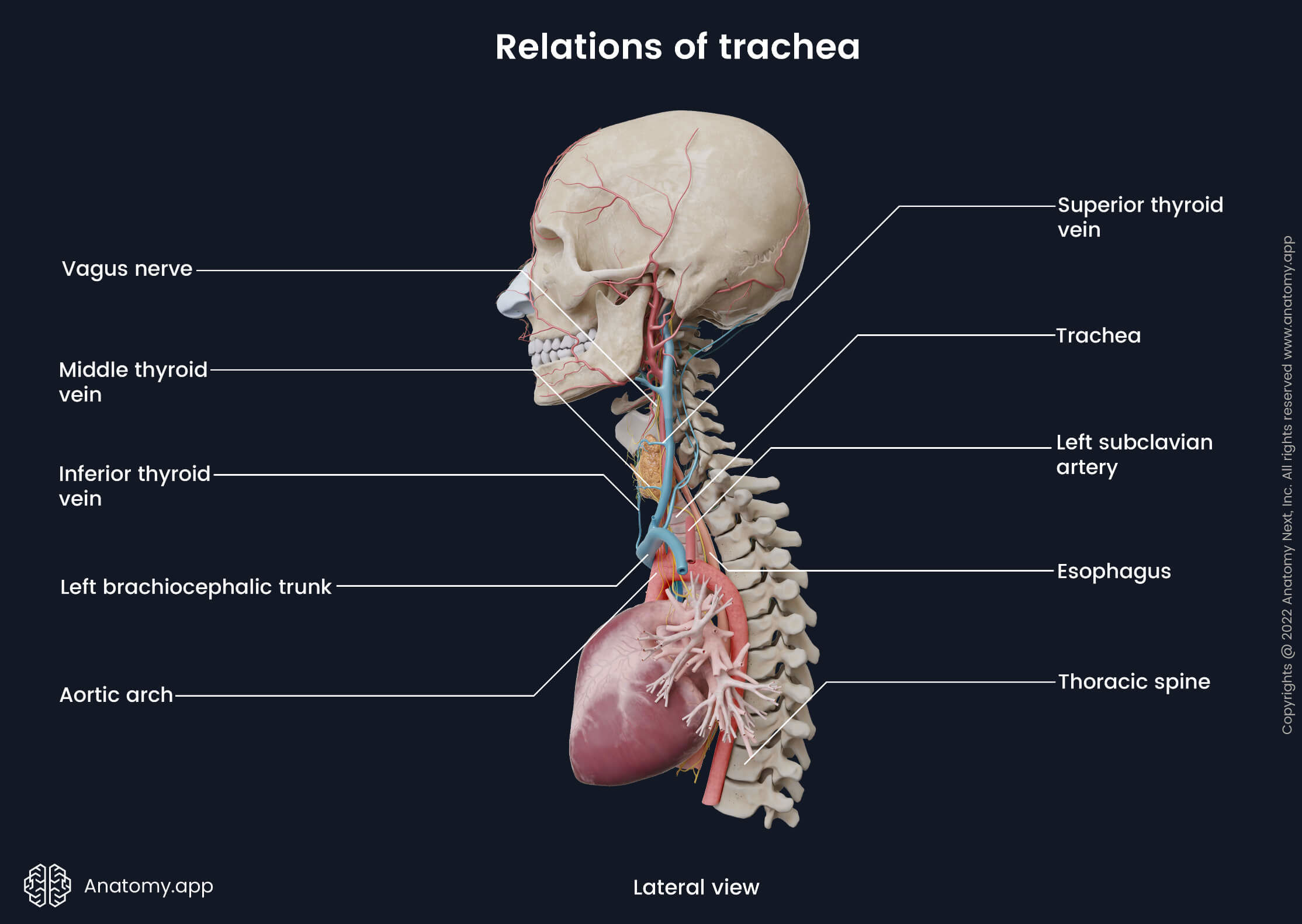
Thoracic part
The thoracic part of the trachea is located in the superior mediastinum. The trachea enters the thorax through the superior thoracic aperture. Anteriorly it borders with the manubrium of the sternum. Lower parts of the infrahyoid muscles mentioned earlier, inferior thyroid vein, thymus (in children) or thymus remnants (in adults) also cover the thoracic portion of the trachea. More inferiorly the anterior surface of the trachea relates to the brachiocephalic trunk, aortic arch, left common carotid artery, left brachiocephalic vein, pretracheal lymph nodes and cardiac plexus.
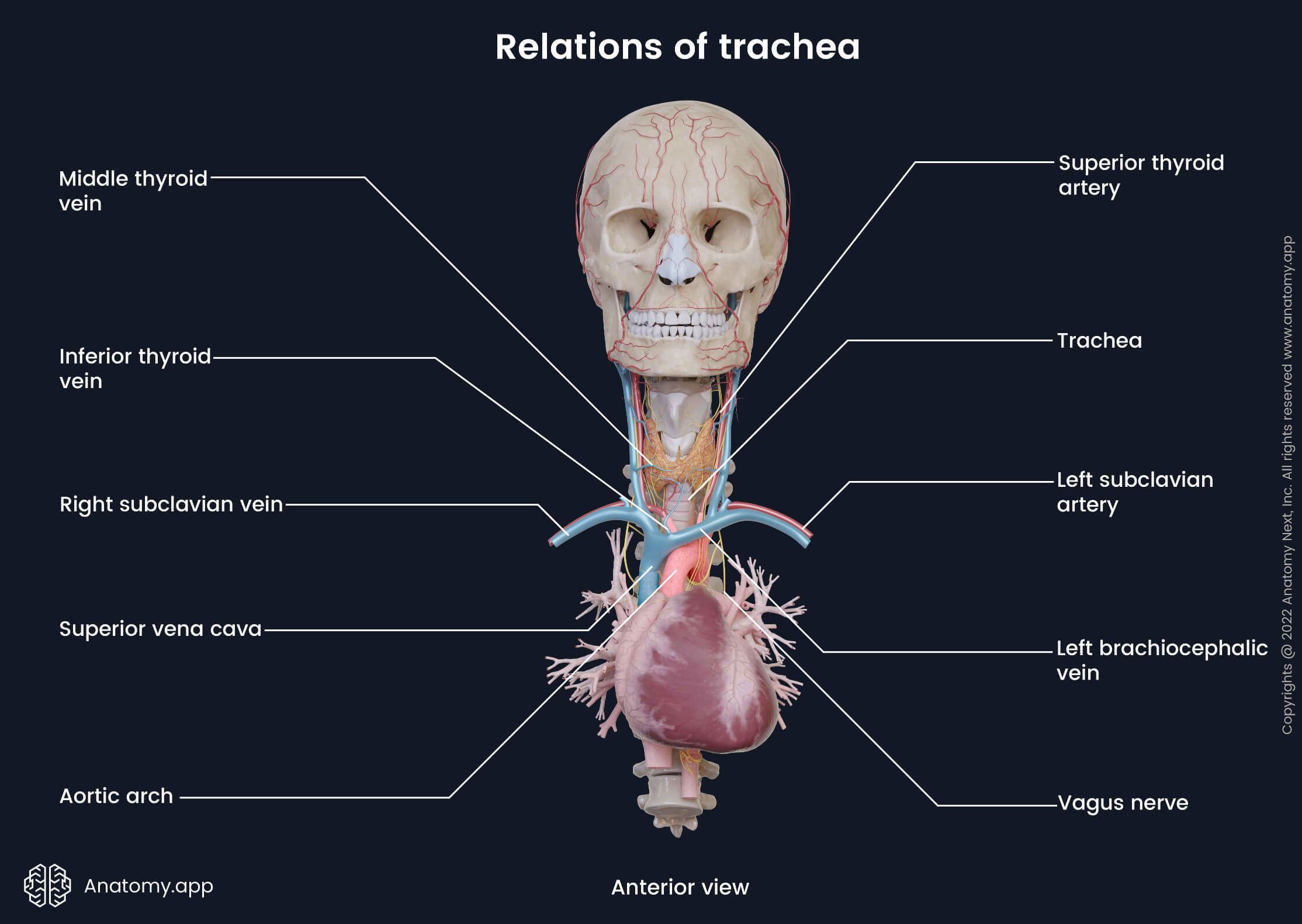
The esophagus is located posteriorly along the tracheal fibromuscular membrane. Between the trachea and esophagus lie venous and nervous plexuses and the retrotracheal group of lymph nodes. Laterally the right side of the trachea is related to the right lung and pleura covering it, right vagus nerve (CN X), right brachiocephalic vein, superior vena cava and azygos vein. The left lateral side of the trachea lies next to the aortic arch, left common carotid and left subclavian arteries. The left recurrent laryngeal nerve arises from the vagus nerve, passes under the aortic arch and then lies in the tracheo-esophageal groove.
Trachea histology
Internally the trachea is lined by a mucosal layer consisting of epithelium and underlying lamina propria - a loose connective layer that supports the epithelium. Under the mucosa lies a submucosal layer made of connective tissue, and it contains smooth muscle cells, mixed tracheal glands, blood and lymph vessels and nerves. The third layer is cartilage and muscle layer composed of smooth muscle cells and hyaline cartilages. And finally, the external layer is adventitia, made of fibroelstic connective tissue.
Mucosal layer
The epithelium of the tracheal mucosa is similar to that of the rest of the lower airways. The inside of the trachea is mainly lined with the respiratory epithelium (pseudostratified columnar ciliated epithelium) containing mucus-secreting goblet cells. The loose connective tissue of the mucosa is composed of many elastic fibers. Six main types of cells are found in the mucosa of the tracheobronchial tree: ciliated columnar, goblet, Clara, brush, basal and neuroendocrine cells.
- Ciliated columnar cells are the primary cells involved in the mucociliary clearance mechanism. Each cell has up to 300 cilia that produce movements. These movements allow foreign particles and pathogens to move out of the airway. The tips of the cilia are immersed into a thick blanket of mucus secreted by the goblet cells and cells of the submucosal glands.
- Goblet cells are found in the trachea and up to smaller bronchi. The apical zone of the goblet cell is filled with secretory vesicles. These cells produce mucinogen - a component of the mucus present in the respiratory tract.
- Clara cells are non-ciliated secretory cells. They produce and secrete surfactant components. Functionally, Clara cells are similar to the type II alveolar cells found in the pulmonary alveoli.
- Brush cells are relatively rare epithelial cell type. They have long apical microvilli. It is thought that these cells act as sensory receptors since they have contact with afferent nerve endings on their basal surfaces.
- Basal cells are small rounded cells. They rest on the basement membrane. Basal cells serve as stem cells that replace other types of epithelial cells (goblet, brush and ciliated columnar cells).
- Neuroendocrine cells are located mainly in the basal part of the respiratory epithelium, and they are a part of a the neuroendocrine system. Neuroendocrine cells are hormone-producing cells that release hormones in response to neural stimuli.
Lymphocytes and mast cells are also found in the airway epithelium. They migrate there from the underlying connective tissue.
- T-lymphocytes found within the trachea mainly come from the mucosa-associated lymphoid tissue (MALT). T-lymphocytes provide immunological functions. They kill and eliminate infected host cells and intracellular microbes, activate other immune cells (macrophages, B cells), regulate immune response and provide cytokine release.
- Mast cells are located in the basal part of the airway epithelium. They contain histamine granules. When triggered by irritants or allergens, they release the granules outside the cell.
Submucosal layer
The submucosa or submucosal layer of the tracheal wall is located under the lamina propria. It contains mixed tracheal glands made up of serous and mucous cells, and they produce mucus that covers the surface of the ciliated epithelium. The connective tissue of the submucosal layer contains long bands of elastin that form a web. This network of elastic fibers helps to adjust the tracheal diameter to the airflow and neck movements.
Cartilage and muscle layer
This layer is also called the fibromusculocartilaginous layer. It includes C-shaped hyaline cartilages and smooth muscle cells. The posterior ends of tracheal cartilages are connected by connective tissue and smooth muscle fibers forming the trachealis muscle. The hyaline cartilages are found in the anterior aspects, while smooth muscle cells are located within the posterior portion of the tracheal wall. Two hyaline cartilages are connected by collagenous and elastic connective tissue that allows the trachea to shorten or lengthen during swallowing or neck movements.
Neurovascular supply of trachea
The trachea receives arterial blood supply mainly from the inferior thyroid and ascending branches of the bronchial arteries. Venous drainage is provided by veins that flow into the inferior thyroid venous plexus and further into the brachiocephalic veins.
And the lymphatic drainage is ensured by lymph vessels that drain into the pretracheal, paratracheal and retrotracheal lymph nodes. From these nodes, lymph is carried next to the deep cervical lymph nodes.
The trachea receives parasympathetic and sensory innervation from the recurrent laryngeal nerves and other branches of the vagus nerve (CN X). Sympathetic innervation originates from the sympathetic trunks and is provided by nerve fibers of the anterior and posterior pulmonary plexuses.
Cough reflex
Coughing is a very important defensive reflex. Normally, it allows inhaled foreign particles to move outward and clear secretions from the airways. In some cases, cough can become pathological and harmful to the airway mucosa.
The foreign particles and mucus in the airways mechanically and chemically trigger the vagus (CN X) and glossopharyngeal (CN IX) nerve fibers. This sensory information through the peripheral nervous system reaches the central nervous system - the spinal cord and the brain. The regions responsible for respiration are located mainly in the medulla oblongata. After processing the information, motor fibers send impulses via the vagus, phrenic and spinal motor nerves to the larynx, diaphragm, thoracic respiratory and abdominal wall muscles.
Mechanically, the coughing process can be divided into three phases:
- Inspiratory phase - characterized by an initial deep inhalation that generates the necessary air volume to expel the foreign particles and mucus;
- Compressive phase - during it a strong contraction of the diaphragm, thoracic and abdominal muscles occurs; combined with a closed glottis, it increases the intrathoracic pressure;
- Expulsive phase - the final phase, in which a sudden opening of the glottis allows a forceful flow of air through the airways. This produces the characteristic coughing sound.
Fun fact: There are specific receptors that can trigger the cough reflex also in the ear and other places of the body, not only the airways. These receptors are thought to be mechanoreceptors that are stimulated by touch or movement. They are found in the external auditory canal, tympanic membrane, paranasal sinuses, pharynx, pleura, pericardium and even stomach.
Coughing is the primary adaptive and defensive mechanism in smoking. If the cough is present for longer than three weeks, it can be referred to as the smoker’s cough. Nevertheless, even after many years of smoking, cessation of tobacco rapidly decreases coughing and improves the overall condition of the airways.
Effects of smoking
Smoking affects not only the trachea but all parts of the tracheobronchial tree and lungs. When the airways are irritated by the tobacco smoke, they become hyper-responsive, and the number of smooth muscle cells rapidly increases. When the epithelium becomes triggered, it increases the overall number of goblet cells. Additionally, these cells start to arise in places they are not originally present - for example, in bronchioles. Usually, these cells are present only in the trachea and larger bronchi. The goblet cells start to produce an excessive amount of mucus to protect the airways, and it, in turn, results in cough reflex.
Smoking and even brief or passive exposure to cigarette smoke affect lung and airway function by secreting inflammatory molecules. It can contribute to developing such lung and airway problems as asthma and chronic obstructive pulmonary disease (COPD). Both mentoned diseases are chronic inflammatory disorders. Their symptoms come mainly from the airway obstruction, and they include chronic cough, shortness of breath, wheezing and frequent respiratory infections.
References:
- Cohen, E. (2021). Cohen’s Comprehensive Thoracic Anesthesia (1st ed.). Elsevier.
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Tamimi, A., Serdarevic, D., & Hanania, N. A. (2012). The effects of cigarette smoke on airway inflammation in asthma and COPD: Therapeutic implications. Respiratory Medicine, 106(3), 319–328. https://doi.org/10.1016/j.rmed.2011.11.003
- Wylam, M. E., Sathish, V., VanOosten, S. K., Freeman, M., Burkholder, D., Thompson, M. A., Pabelick, C. M., & Prakash, Y. S. (2015). Mechanisms of Cigarette Smoke Effects on Human Airway Smooth Muscle. PLOS ONE, 10(6), e0128778. https://doi.org/10.1371/journal.pone.0128778
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app