- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
Liver
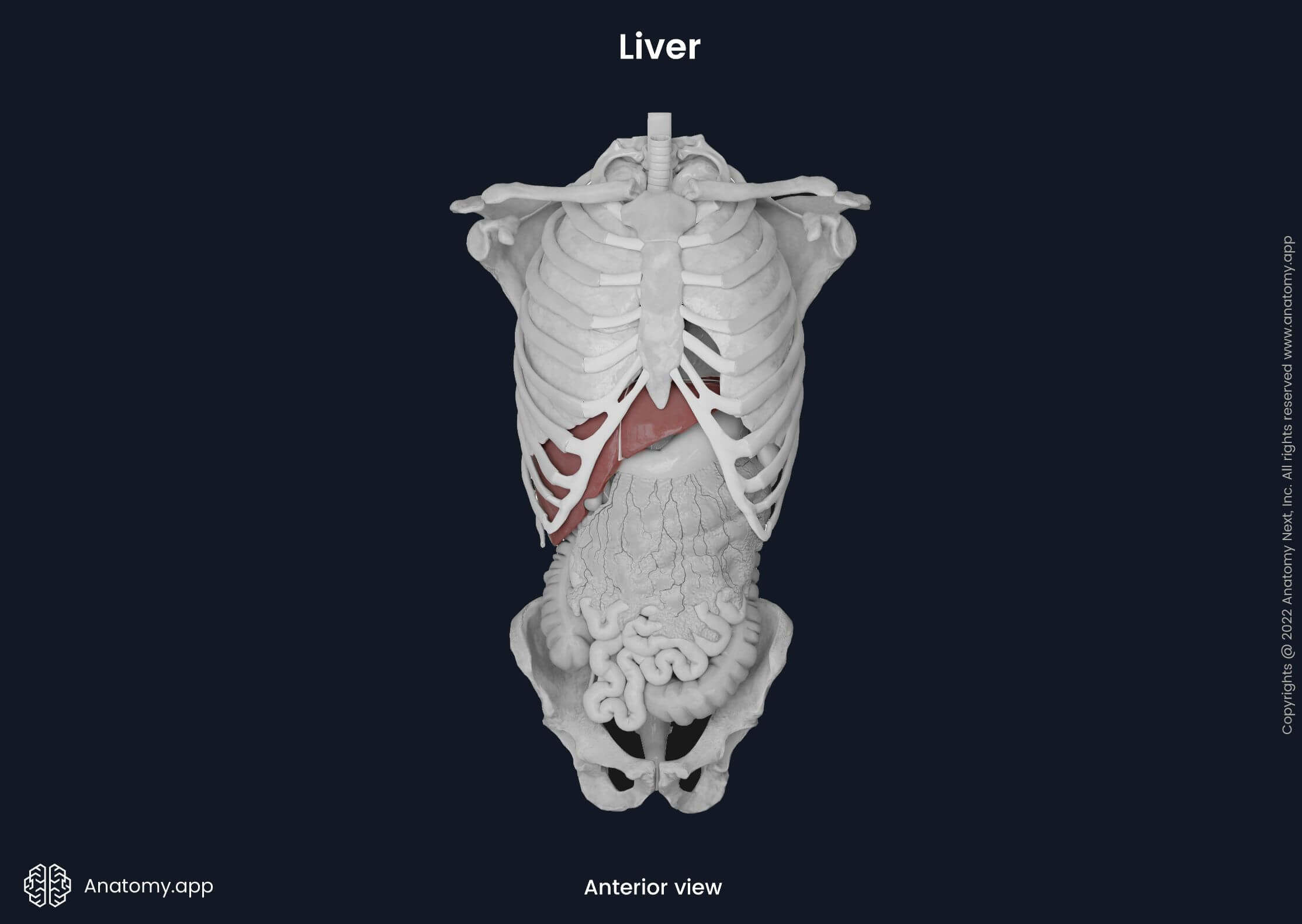
The liver (Latin: hepar) is a wedge-shaped accessory organ of the gastrointestinal tract and the largest organ in the abdominal cavity. It is also the most prominent gland and second-largest organ in the human body after the skin. Most of the liver is located inside the rib cage. Its base is positioned below the xiphoid process of the sternum (epigastric region) and on the right side of the upper abdomen (right hypochondriac region). The apex of the liver occupies the left side of the upper abdomen (left hypochondriac region). The liver weighs around 1.2 - 1.6 kg. Its weight gradually decreases with aging. The liver is an important metabolic organ responsible for the maintenance of homeostasis, immune defense and nutrition, among many other functions.
Liver anatomy
The liver is located under the diaphragm. The lower margin of the liver corresponds to the lower margin of the rib cage and lower ribs. Almost the entire liver is encapsulated within the visceral peritoneum, except for the gallbladder fossa, porta hepatis and the bare area, where the liver is in direct contact with the diaphragm. Beneath the peritoneum, the liver is covered by a fibrous capsule known as Glisson’s capsule. This capsule also covers each structure of the porta hepatis that enters the liver.
Liver surfaces
Although the liver can be viewed from different aspects such as superior, inferior, anterior and posterior, only two major surfaces are typically distinguished - diaphragmatic and visceral. Both surfaces are separated by a sharp inferior border.
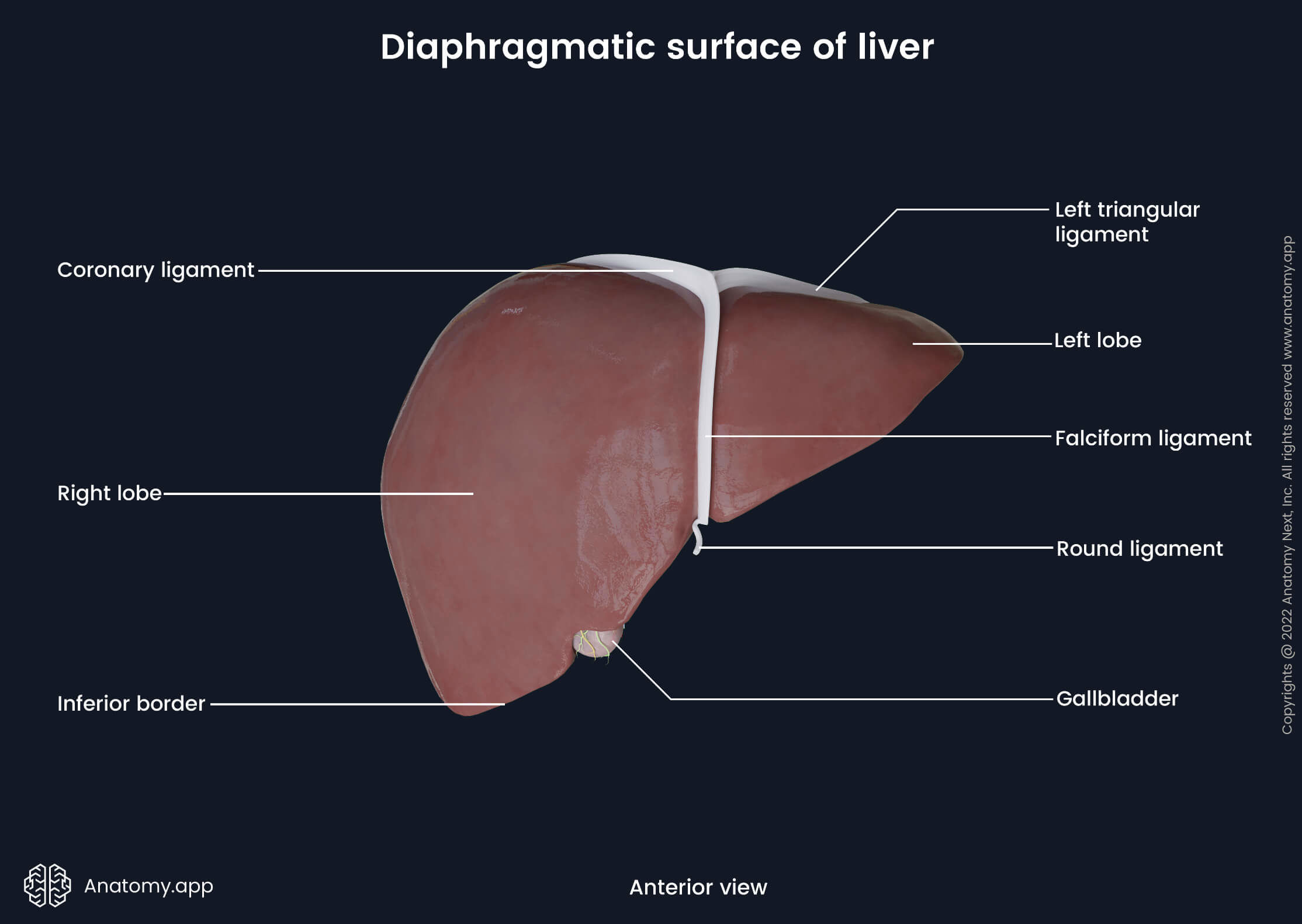
Diaphragmatic surface
The diaphragmatic surface is a smooth and convex antero-superior surface facing the inferior surface of the diaphragm. It is covered by the visceral peritoneum, except the bare area located on the supero-posterior aspect of the surface. The bare area is in direct contact with the diaphragm.
The anterior aspect of the diaphragmatic surface is mainly covered by the anterior parts of the diaphragm. On the right side, the diaphragm and peritoneum separate the anterior surface of the liver from the pleura and sixth to eleventh ribs with their respective cartilages. On the left side, the anterior surface corresponds to the seventh and eighth costal cartilages.
The superior aspect of the diaphragmatic surface lies directly inferior to the diaphragm under its right dome. The liver and diaphragm are separated by the peritoneum. However, the superior surface also directly contacts the diaphragm in a small triangular-shaped area (bare area) where the peritoneum is absent. The bare area is marked by the two layers of the coronary ligament.
Visceral surface
The visceral surface of the liver is a relatively flat and irregularly-shaped postero-inferior surface that faces various abdominal organs. It is also covered by the visceral peritoneum, except at the porta hepatis and fossa of the gallbladder. It communicates with the right kidney and its suprarenal gland, right colic flexure, transverse colon, duodenum, gallbladder, esophagus and stomach.
The middle part of the visceral surface presents with an H-shaped group of fissures and fossae. The transverse fissure (representing the crossbar of the letter H) is formed by the porta hepatis. The left limb of the H is composed of two deep sagittal fissures for two ligaments - venous and round ligaments. And finally, the right limb of the letter H is formed by impressions of the inferior vena cava and gallbladder.
The inferior aspect of the visceral surface communicates with the previously mentioned abdominal organs. Also, it contains previously described fissures and fossae that together form an H shape. The quadrate lobe lies anterior to the porta hepatis, while the caudate lobe is located posterior to it.
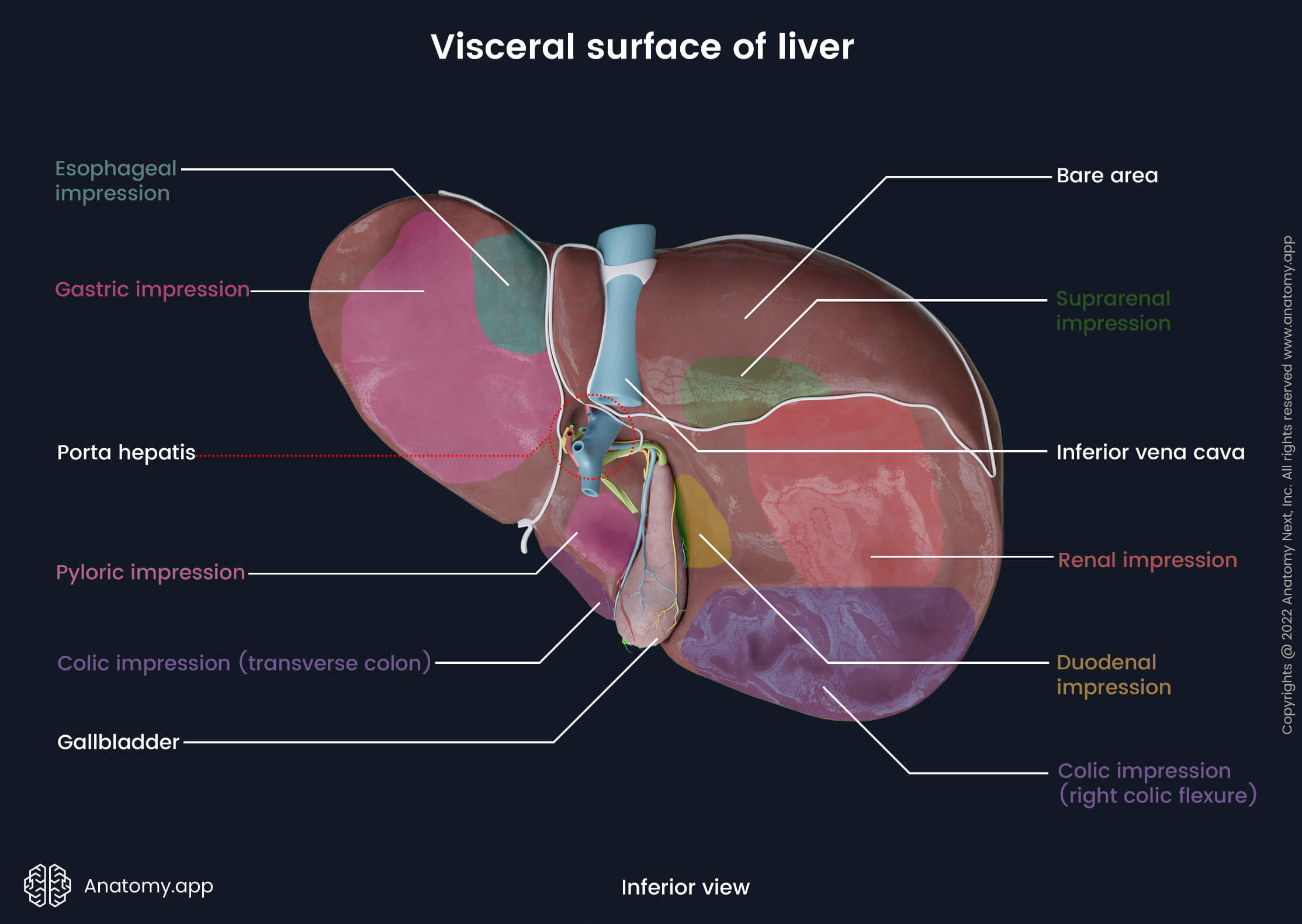
The quadrate lobe relates to the pylorus of the stomach, transverse colon and a small part of the lesser omentum. The inferior surface of the left lobe contains gastric and esophageal impressions. Also, it communicates with the lesser omentum. The right lobe on the right side of the gallbladder has a colic impression created by the right flexure of the colon. Superior and next to it is the duodenal impression for the descending part of the duodenum. Superior to both previously mentioned areas are the renal and suprarenal impressions that correspond to the right kidney and suprarenal gland.
The posterior aspect of the visceral surface is convex and lies adjacent to the vertebral column. The majority of the posterior surface attaches to the diaphragm. On the posterior surface between the right and caudate lobes lies a groove for the inferior vena cava. Sometimes this groove is referred to as a fossa because it is more like a deep depression. On the left side of the groove, the caudate lobe of the liver can be distinguished. It relates to the diaphragm. A fissure for the ligamentum venosum is located between the caudate lobe and the left lobe of the liver.
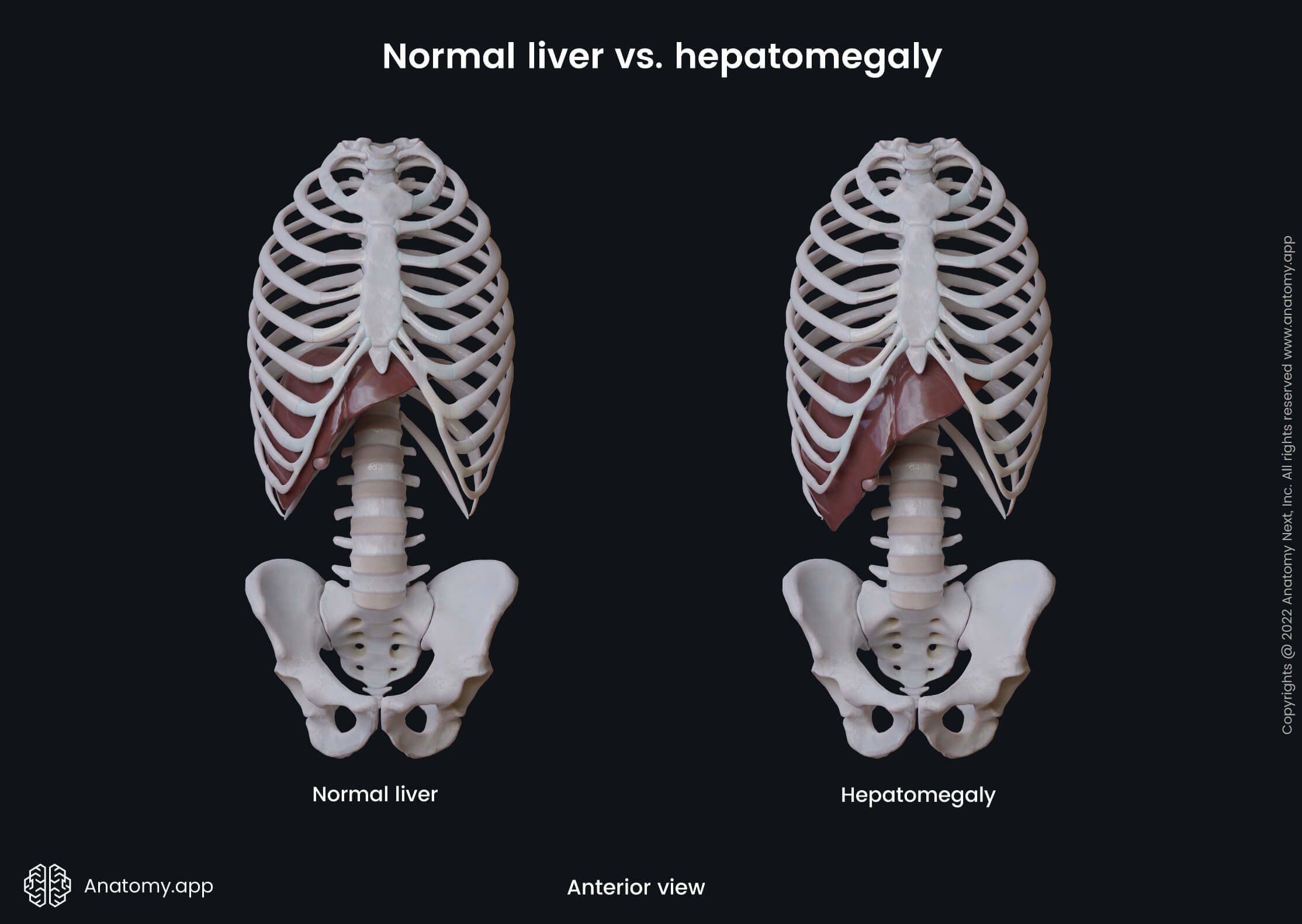
Clinical note: In a healthy individual, the liver can be examined by touch (palpated) at the midline (epigastric region) of the abdomen just below the infrasternal angle and xiphoid process. Here the inferior border of the liver lies the closest to the anterior abdominal wall. If the liver becomes enlarged, it can be palpated under the costal arch and way below the infrasternal angle in the epigastric region.
Anatomical and functional division of liver
The liver can be viewed from two different perspectives - anatomical and functional. Anatomically, it is divided into four lobes based on the visual appearance of the liver. In contrast, the current understanding of the functional anatomy of the liver encompasses two models - a French model and an American one. In the French model, the liver is divided based on the distribution of portal and hepatic veins. On the other hand, the American model divides it according to the branching patterns of bile ducts.
Nowadays, the most widely used system for functional division of the liver is the French model with the Couinaud classification. In 1957 a French surgeon named Claude Couinaud described a classification of eight independent functional units (segments) of the liver according to the branching pattern of the portal vein and hepatic veins within the hepatic parenchyma (functional tissue of the liver). All segments are provided by a vascular inflow, outflow and biliary drainage as each of them contains a branch of the portal vein, hepatic artery and biliary duct. The outflow happens via the hepatic veins found in the periphery of the segments. Find out more about the segments and sectors further in the article.
Liver lobes
As previously mentioned, the liver is divided into four anatomical lobes - right, left, caudate and quadrate. The right lobe is the largest of all. Anteriorly, it is separated from the left lobe by the falciform ligament, posteriorly - by a fissure for the ligamentum venosum and inferiorly by a fissure for the round ligament (ligamentum teres hepatis). The left lobe of the liver is smaller and thinner than the right one. It is located on the left side of the falciform ligament. The apex of the left lobe extends into the left hypochondriac region.
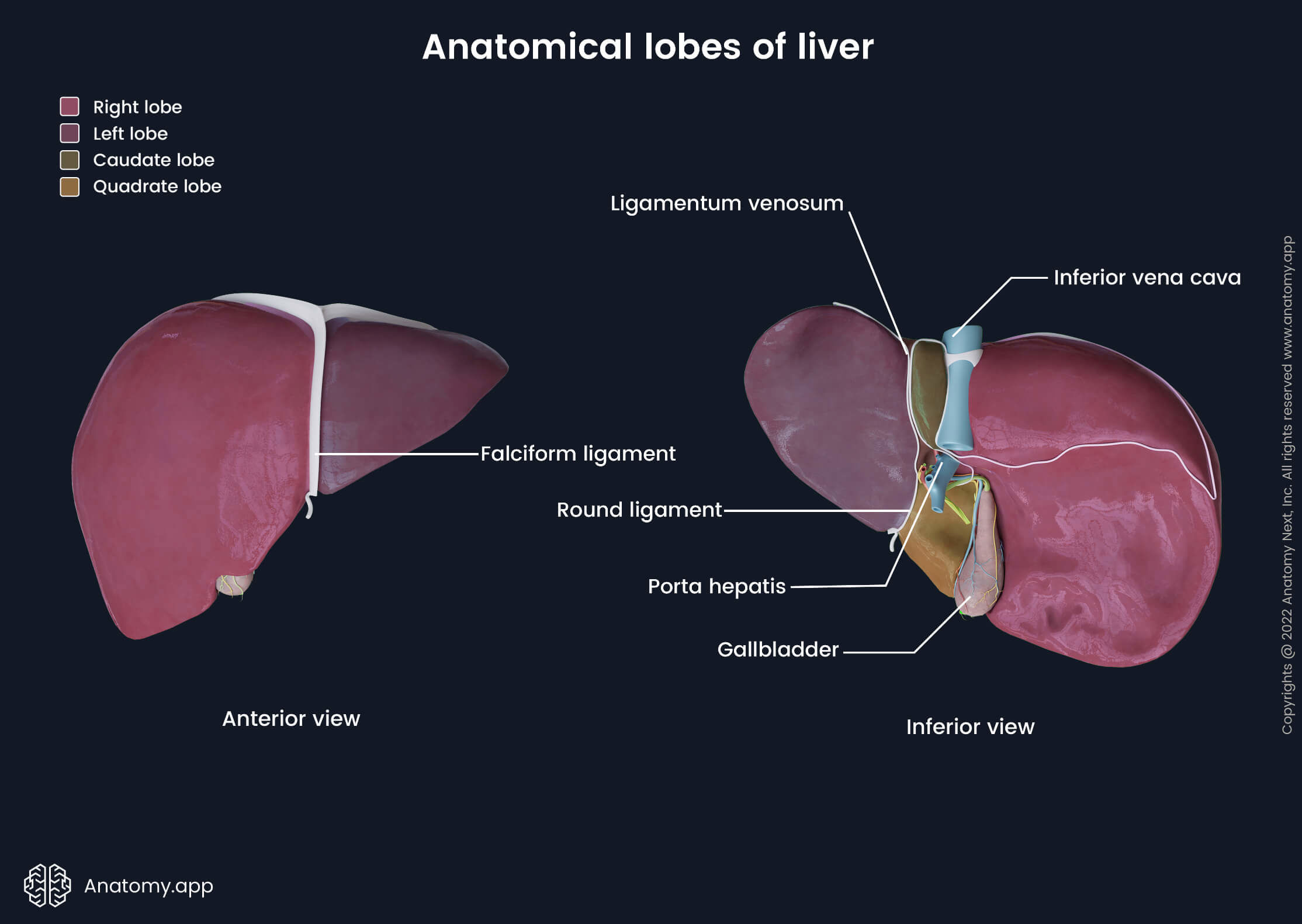
The quadrate lobe can be seen on the visceral surface of the liver. It is marked by the porta hepatis (posteriorly), gallbladder fossa (on the right), fissure of the round ligament (on the left) and inferior border of the liver (anteriorly). The caudate lobe can also be seen on the visceral surface of the liver. It is bounded by the porta hepatis inferiorly, a groove for inferior vena cava on the right, and a fissure for the ligamentum venosum on the left. Superior to it is the diaphragmatic surface of the liver.
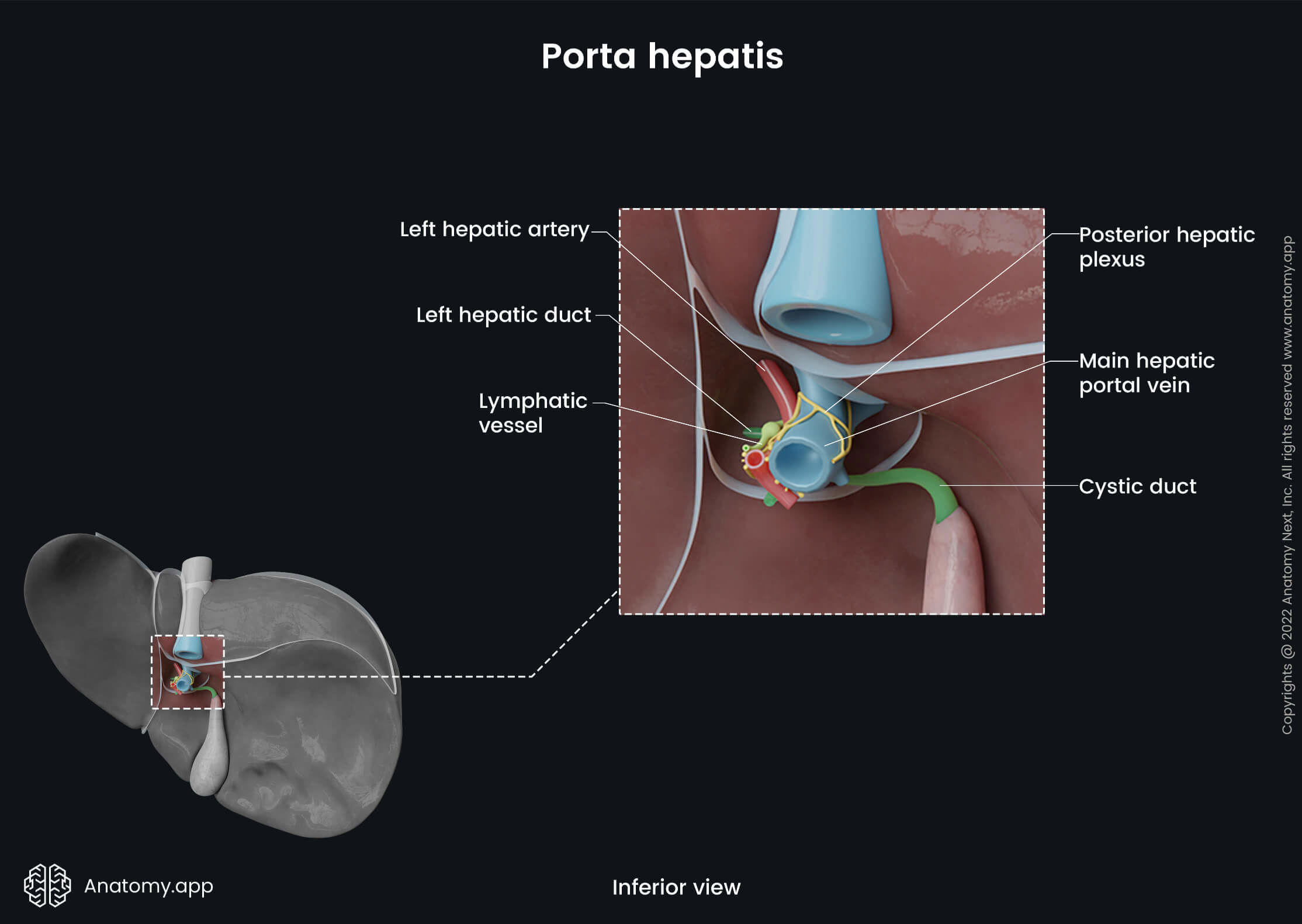
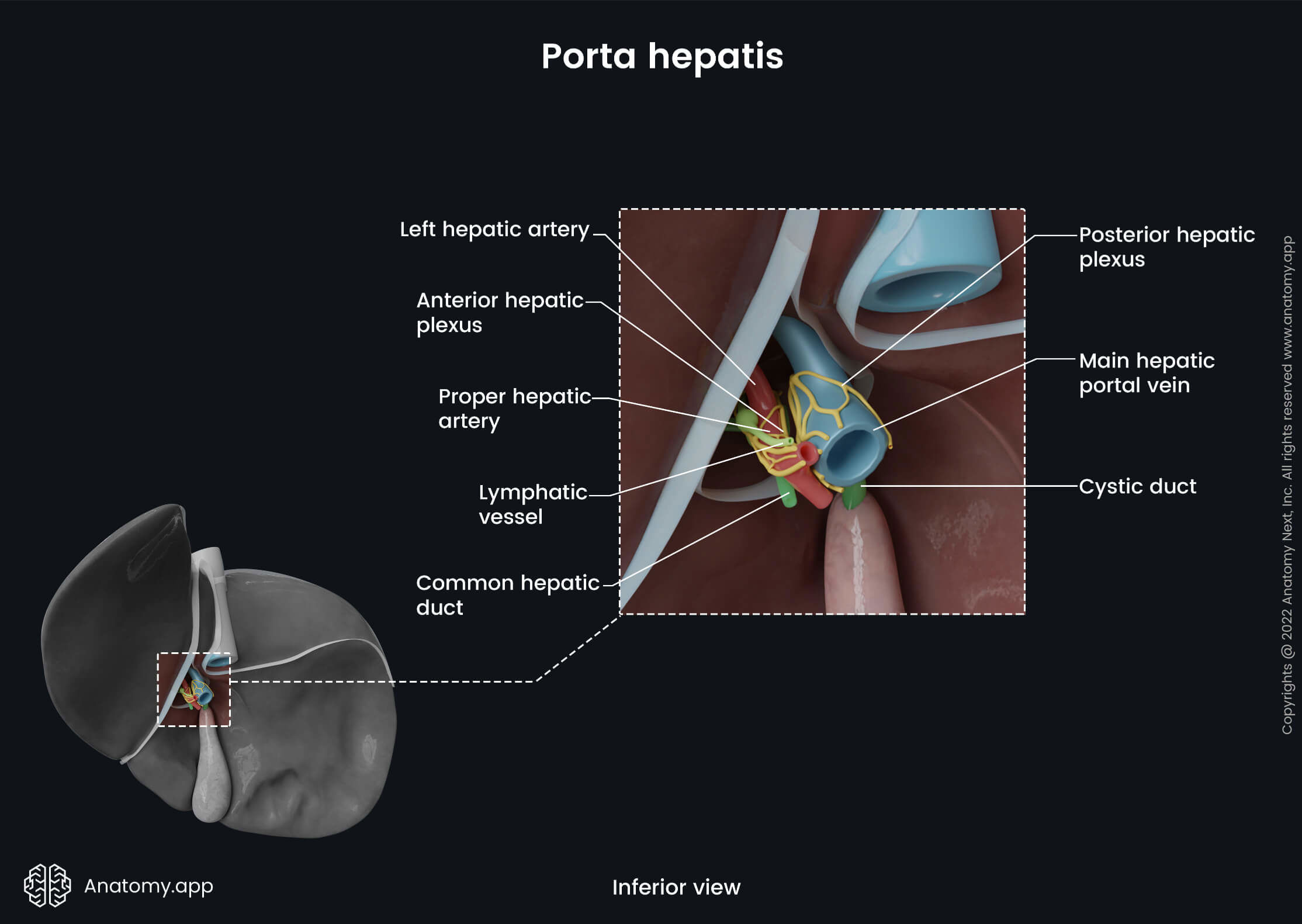
On the visceral surface of the liver between the quadrate and caudate lobes is a deep central transverse fissure called the porta hepatis. Here the main neurovascular structures (except hepatic veins) and hepatic ducts enter and leave the liver. The porta hepatis contains the portal vein, hepatic artery proper, hepatic nervous plexuses, common hepatic duct and lymph vessels. The gallbladder lies on the visceral surface of the right lobe between the right lobe and quadrate lobe.
Functional division
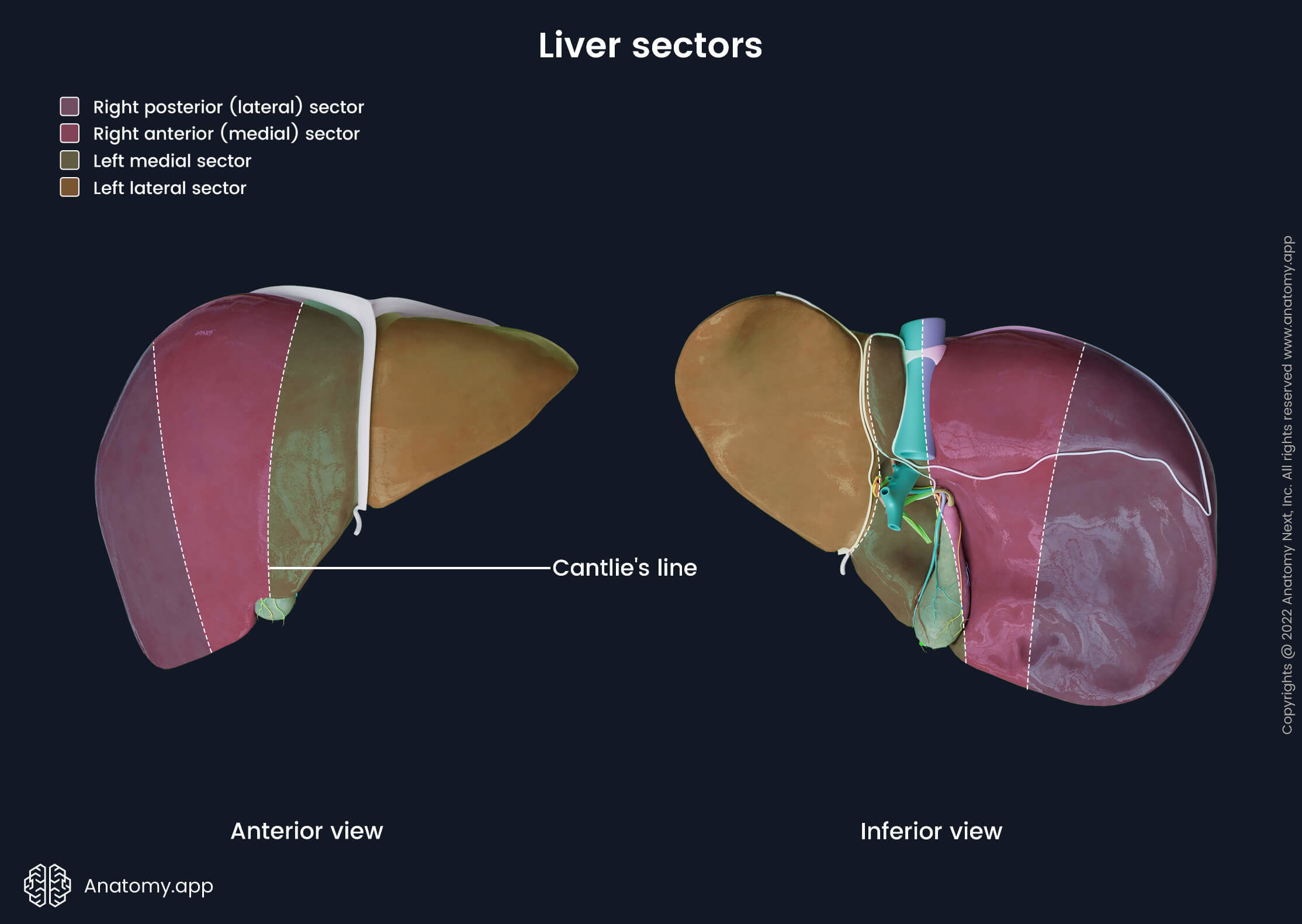
Functionally, the liver can be divided into four sectors according to the distribution of the hepatic veins and areas drained by them. Each sector is usually divided into two segments. The intersectoral planes between these sectors are termed portal fissures. They are not visible externally on the liver surfaces and are only identifiable in the parenchyma of the liver. The three principal hepatic veins run through these fissures.
Liver sectors and segments
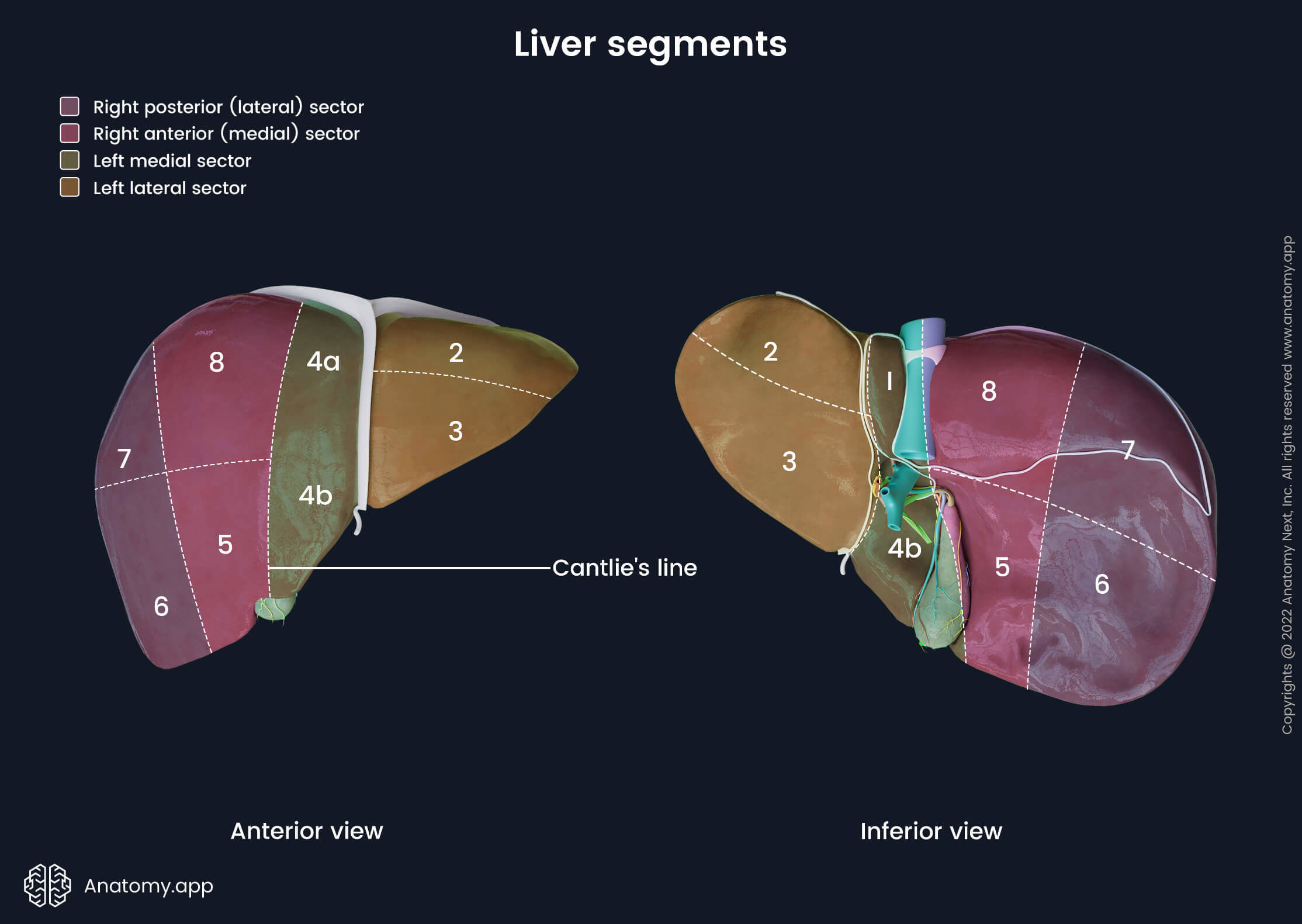
The liver consists of four sectors and eight segments. To understand the arrangement of all sectors and segments, one should first know the difference between the functional and anatomical lobes of the liver. As you already know, the liver has four anatomical lobes. At the same time, it is composed of two functional lobes - left and right. The left functional lobe contains the anatomical left, caudate and quadrate lobes. The border between the right and left functional lobes is marked by the inferior vena cava and gallbladder. The imaginary borderline between both functional lobes in abdominal surgery is known as the Cantlie’s line.
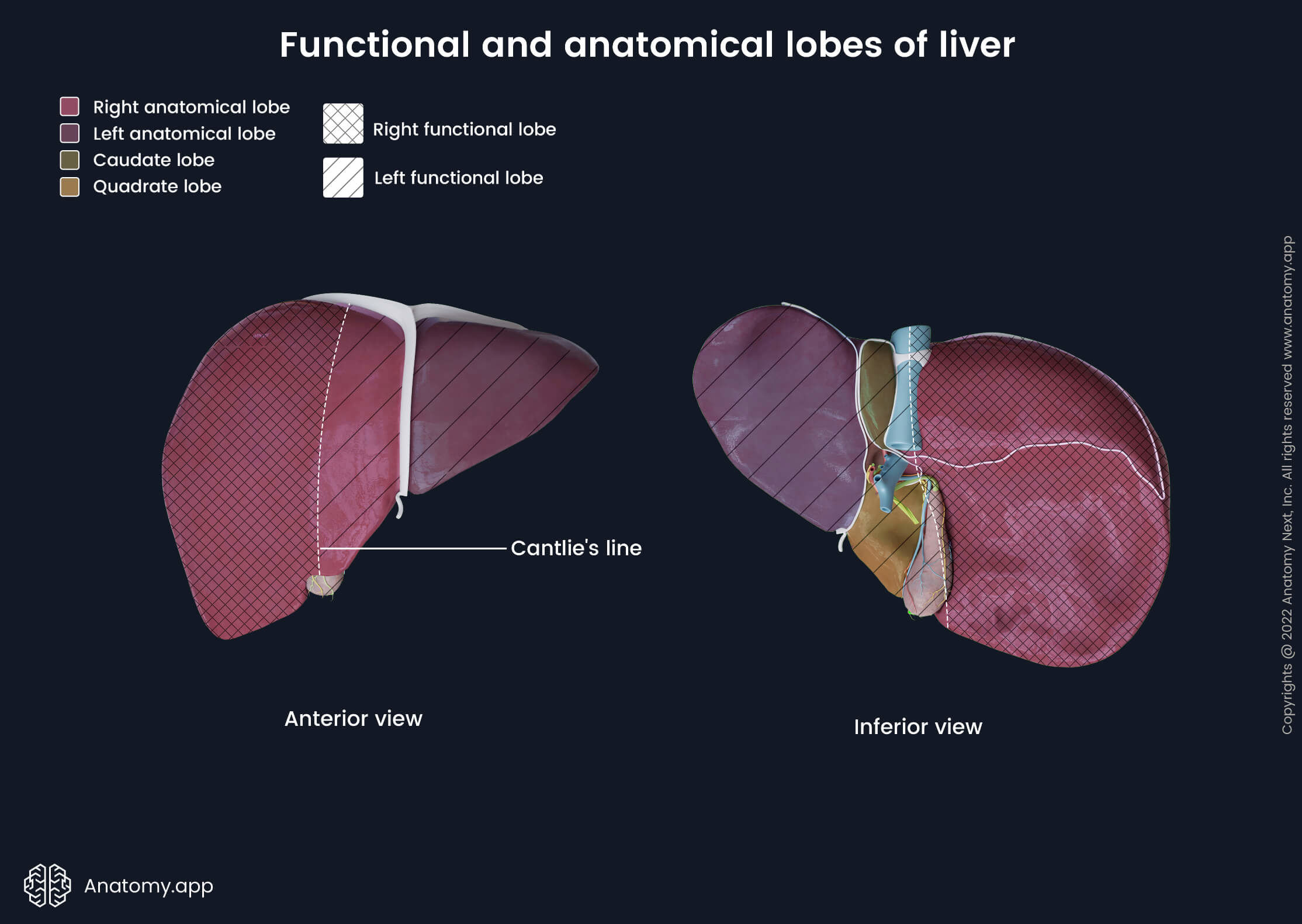
Each functional hepatic lobe is divided into two sectors. The right lobe is composed of the right anterior (medial) and right posterior (lateral) sectors, while the left lobe contains the left lateral and left medial sectors. Both left sectors can be separated along the attachment line of the falciform ligament and fissures for the ligamentum venosum and round ligament. To sum up, the left medial sector is composed of anatomical caudate and quadrate lobes. The left lateral sector lies lateral to it. In contrast, there are no such visible landmarks to distinguish both right sectors. Instead, both are usually divided by an imaginary oblique line drawn anteroposteriorly from the upper-middle aspect of the right functional lobe to the inferior border of the liver.
Each sector can be further subdivided into one or two segments. Originally liver segments were numbered using Roman numerals I to VIII, but nowadays, instead of the Roman numerals, the Arabic numerals 1 to 8 are used. The right anterior (medial) sector includes segments 5 and 8. The right posterior (lateral) sector contains segments 6 and 7. The left medial sector has segments 4 and 1. And finally, the left lateral sector includes segments 2 and 3. The numbering of the segments goes in a clockwise direction. It starts with the caudate lobe (segment 1) and continues from the left to the right side of the liver.
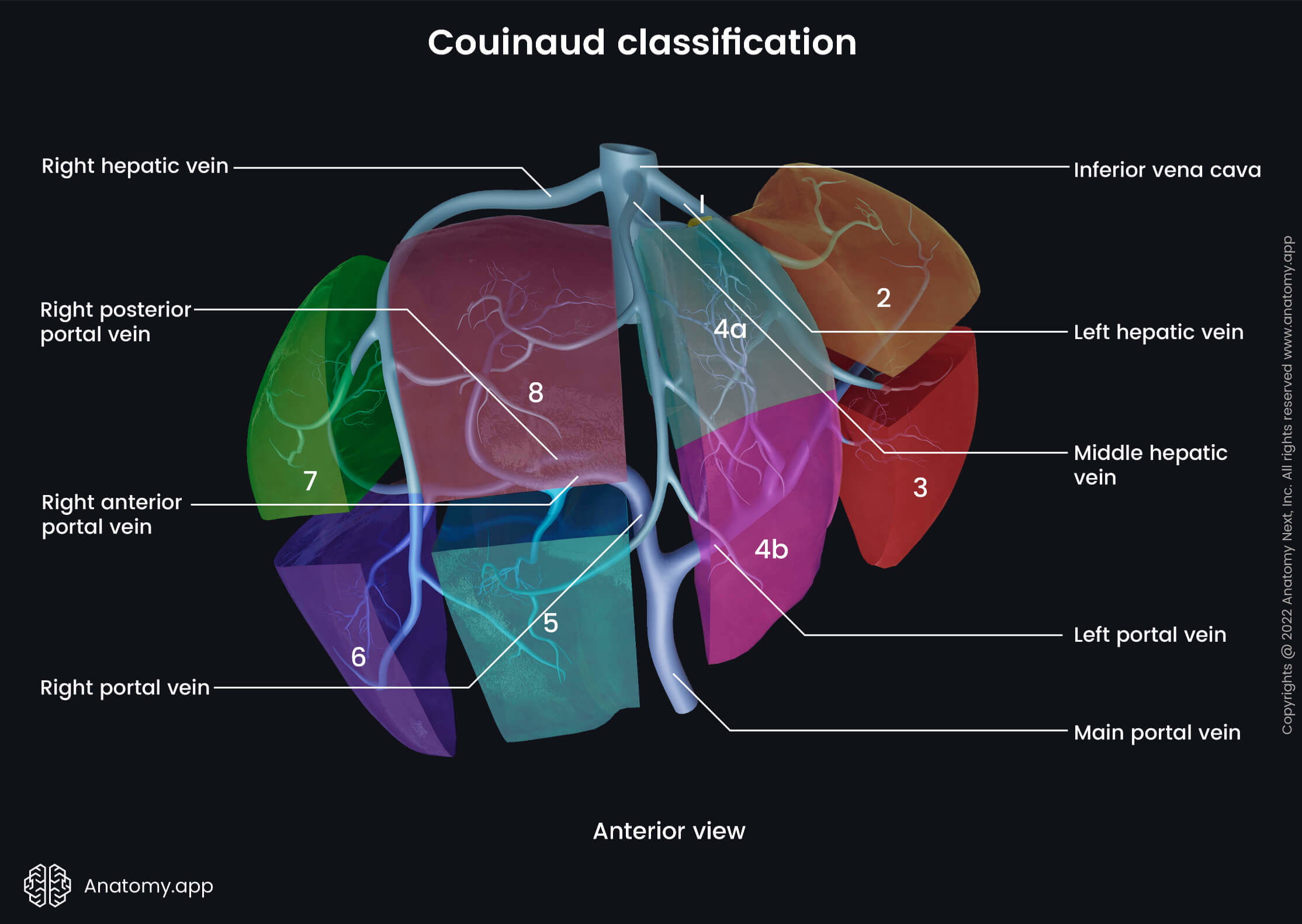
Now that you know the arrangement of the liver let’s take a deeper look at the Couinaud classification. As previously described, the liver is divided into eight independent functional segments according to the branching pattern of the portal vein and hepatic veins. The liver contains several planes according to the French model - three vertical and one horizontal. Hepatic veins represent vertical planes and divide the liver into sectors. The horizontal plane is marked by the portal vein that divides the liver into lower (3, 4b, 5, 6) and upper (2, 4a, 8, 7) segments. It is easier to understand where each liver segment is drained by knowing the arrangement of the main hepatic veins. The middle hepatic vein separates the left and right functional lobes. The left hepatic vein divides the left functional lobe into left medial and left lateral segments, while the right hepatic vein divides the right functional lobe into right anterior (medial) and right posterior (lateral) segments. The knowledge of the Couinaud classification is primarily used in abdominal surgery.
- Segment 1 corresponds to the caudate lobe and additional areas of its neighboring parenchyma. It is supplied by branches of both the right and left portal veins. Segment 1 neighbors anteriorly with segment 4. It surrounds the inferior vena cava and via small hepatic veins drains directly into it. Surgeons divide this segment into three parts - the caudate process, Spiegel’s lobe (caudate lobe and papillary process) and the paracaval part.
- Segment 2 is the superior segment of the left lateral sector. It usually drains via the superior hepatic vein into the left hepatic vein.
- Segment 3 is the inferior segment of the left lateral sector. This segment drains mainly into the left hepatic vein.
- Segment 4 corresponds to the left medial sector and borders posteriorly with segment 1. Usually, this segment is divided into two subsegments - 4a (superiorly) and 4b (inferiorly). Segment 4 typically drains into the middle hepatic vein and sometimes also into the left hepatic vein.
- Segment 5 is the inferior segment of the right anterior (medial) sector. Venous drainage occurs via the right and middle hepatic veins, or the blood can flow directly into the inferior vena cava.
- Segment 6 is found in the inferior aspect of the right posterior (lateral) sector. It is drained into the right hepatic vein, or similar to the segment V - directly into the inferior vena cava.
- Segment 7 lies in the superior aspect of the right posterior (lateral) sector. Venous drainage is provided by the right hepatic vein.
- Segment 8 is the superior part of the right anterior (medial) sector. It drains into the right and middle hepatic veins.
Portal fissures
In total, the liver has three major and three minor portal fissures. The major portal fissures include the main, left and right portal fissures. The minor portal fissures can be observed on the external surface of the liver as cleft-like structures. These are the venous and umbilical fissures and the so-called Rouviere’s sulcus. One should know that these fissures are used in abdominal surgery and while studying functional anatomy rather than gross anatomy of the liver.
The main portal fissure extends from the inferior border of the liver at the fossa of the gallbladder along the midpoint of the inferior vena cava to the superior aspect of the diaphragmatic surface. The middle hepatic vein runs through it. The main portal fissure divides the liver into two functional lobes and is surrounded by segments 5 and 8 on the right and segments 4 and 1 on the left side.
The right portal fissure divides the right functional lobe into right anterior (medial) and right posterior (lateral) sectors. It extends diagonally through the right lobe from the lateral part of the inferior margin of the liver along the course of the right hepatic vein. It is surrounded by segments 5 and 8 on the left and segments 6 and 7 on the right side. The right hepatic vein passes through the right portal fissure.
The left portal fissure separates the left functional lobe of the liver into the left medial (anterior) and left lateral (posterior) sectors. It runs from the midpoint of the inferior margin between the left triangular and falciform ligaments to the site where the left and middle hepatic veins merge. In this fissure, the left hepatic vein is located. The left portal fissure divides the left medial (anterior) sector from the left lateral (posterior) sector. Segment 2 lies posteriorly, while segment 3 is located anteriorly.
The venous fissure is a continuation of the umbilical fissure on the visceral surface of the liver. It contains the ligamentum venosum. The venous fissure separates the caudate lobe from segment 4.
The umbilical fissure is marked by the attachment of the falciform ligament and runs parallel to it. The umbilical fissure contains the round ligament, umbilical fissure vein (a tributary of the left hepatic vein), bile ductules forming the left hepatic duct and terminal branches of the left hepatic artery. The umbilical fissure separates segments 3 and 4.
The Rouviere’s sulcus (fissure of Gans or incisura hepatis dextra) is found in around 80% of individuals. It is located on the visceral surface of the right lobe posterior to the gallbladder fossa. Posteriorly it borders with segment 1 and anteriorly - with the fossa of the gallbladder.
Liver ligaments
Through different attachments and ligaments, the liver is connected to the diaphragm, anterior wall of the abdomen and adjacent abdominal organs. The liver contains the following ligaments:
- Falciform ligament
- Round ligament of the liver (ligamentum teres hepatis)
- Coronary ligament
- Right and left triangular ligaments
- Hepatogastric ligament
- Hepatoduodenal ligament
- Ligamentum venosum
The falciform ligament attaches the liver to the anterior abdominal wall and diaphragm. It is composed of two layers or leaves, and they extend on the diaphragmatic surface of the liver between the right and left lobes. The falciform ligament attaches to the posterior (visceral) aspect of the anterior abdominal wall and inferior surface of the diaphragm.
The right leaf of the falciform ligament is continuous with the coronary ligament laterally. The left leaf continues medially as the left triangular ligament. The falciform ligament descends between both lobes reaching the inferior border of the liver. The inferior border of the falciform ligament is free and does not have any attachments. Here, the round ligament of the liver (also known as the ligamentum teres hepatis) is found. It is an obliterated remnant of the left umbilical vein that functions during the fetal period. It extends from the inferior aspect of the falciform ligament to the visceral surface of the liver. The round ligament of the liver is an important landmark in abdominal surgery.
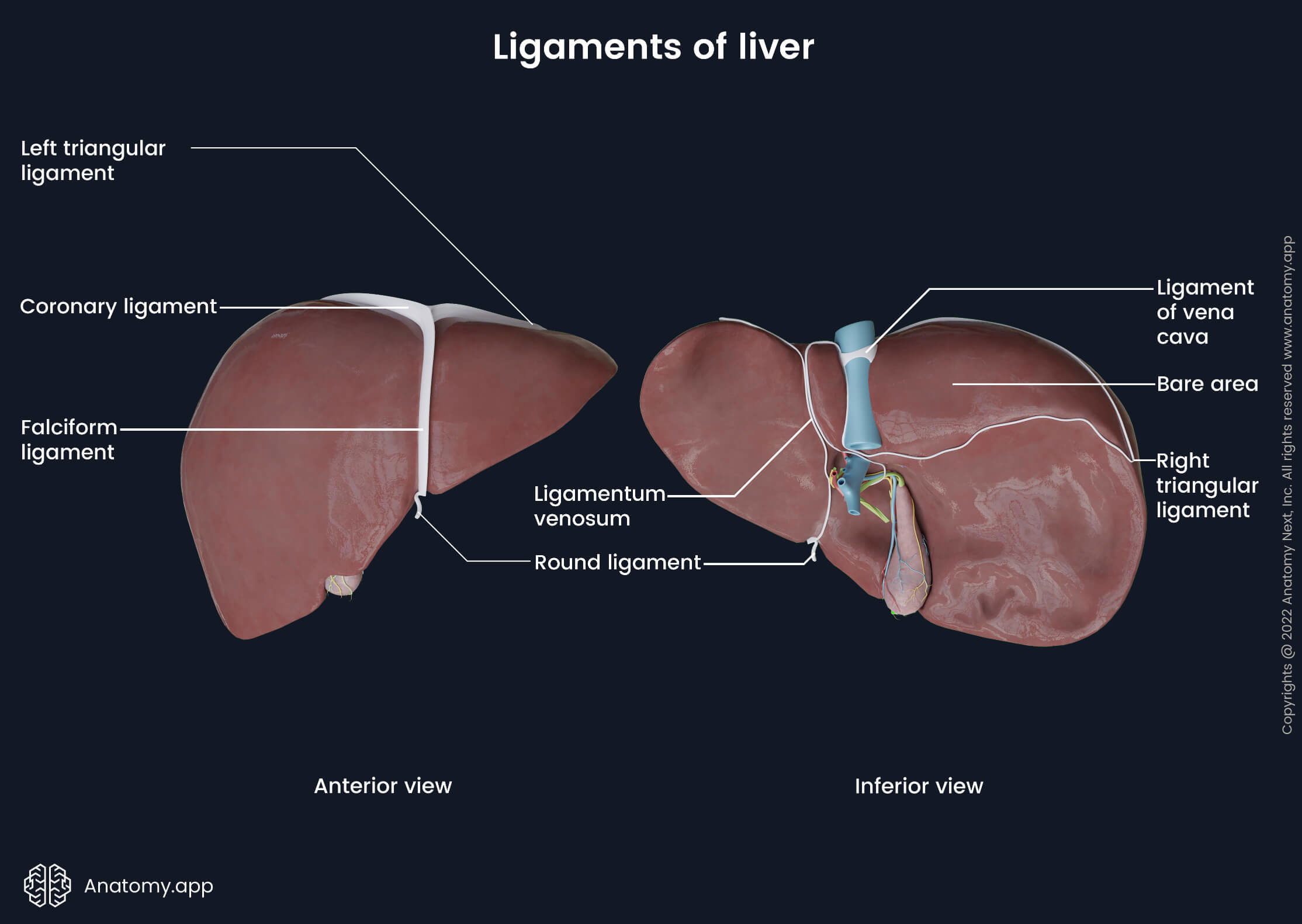
The coronary ligament is a reflection of the peritoneum. It extends from the inferior surface of the diaphragm to the superior and posterior aspects of the right lobe of the liver. The coronary ligament consists of two layers - anterior (superior) and posterior (inferior). On the diaphragmatic surface of the liver between both layers of the ligament is a large triangular-shaped area (so-called “bare area”) where the liver is not covered by the peritoneum.
Both layers of the coronary ligament form the right and left triangular ligaments on each side. The anterior layer of the ligament runs superiorly on the diaphragmatic surface of the liver and connects it with the inferior surface of the diaphragm. The posterior layer of the ligament connects the visceral surface of the liver to the posterior abdominal wall, right suprarenal gland and right kidney.
As previously mentioned, the liver contains two triangular ligaments - right and left. Both are continuations of the coronary ligament. The right triangular ligament is formed by both layers of the coronary ligament. It is short and has a border with the bare area of the liver. The left triangular ligament is also formed by both layers of the coronary ligament. It consists of two layers and extends along the superior aspect of the left lobe of the liver. The anterior leaf continues as the left layer of the falciform ligament. The posterior leaf continues as the lesser omentum.
The lesser omentum is a double layer of the peritoneum that runs from the inferior surface of the liver to the lesser curvature of the stomach and proximal part of the duodenum. It consists of the hepatogastric ligament (attaches the liver to the stomach) and hepatoduodenal ligament (attaches the liver to the duodenum). The lesser omentum has a free margin between the porta hepatis and duodenum, which encloses the structures of the porta hepatis. Superiorly the left layer of the lesser omentum continues as the posterior layer of the left triangular ligament. The right layer continues as the coronary ligament.
The ligamentum venosum is an obliterated remnant of the ductus venosus that functions during fetal circulation. In the fetus, ductus venosus is a shunt that allows blood to bypass the liver as it connects the umbilical vein directly with the inferior vena cava.
Neurovascular supply of liver
Vasculature of liver
The liver receives a dual blood supply coming from the hepatic artery and portal vein. The portal vein provides around 70-75% of the blood directed to the liver. It contains blood poor in oxygen but rich in nutrients absorbed from the small intestines. The systemic arterial blood supply occurs via the hepatic artery, and it constitutes around 25-30% of the blood flow. The hepatic artery carries blood rich in oxygen. Venous drainage of the liver occurs via the hepatic veins that drain into the inferior vena cava.
Blood supply
The systemic arterial blood supply is provided by the hepatic artery. It originates from the celiac trunk, ascends through the free margin of the lesser omentum to reach the liver and enters the liver via the porta hepatis. The hepatic artery is divided into two segments: the common hepatic artery (extending from the celiac trunk to the origin site of the gastroduodenal artery) and the proper hepatic artery (from the origin site of the gastroduodenal artery to the porta hepatis). The proper hepatic artery bifurcates into two branches - the left and right hepatic arteries - at the hilum of the liver.
The left hepatic artery runs towards the umbilical fissure and left lobe of the liver. It supplies segments 2, 3 and 4. The left hepatic artery gives off the middle hepatic artery that supplies segment 4. The right hepatic artery ascends to the right aspect of the liver, going posterior to the common hepatic duct. It gives off a branch - cystic artery. The cystic artery supplies the gallbladder and cystic duct. The right hepatic artery then continues further and reaches the right lobe of the liver, where it divides into the anterior and posterior segmental arteries. The anterior branch supplies segments 5 and 8 and usually gives an additional branch to segment 1. The posterior branch supplies segments 6 and 7.
As mentioned above, the liver is also supplied by the portal vein. The portal venous system collects nutrient-rich blood from the gastrointestinal tract and its accessory organs and carries it to the liver. The main hepatic portal vein arises behind the neck of the pancreas. It is formed by the confluence of two veins - the superior mesenteric and splenic veins. Also, the inferior mesenteric vein may join either the superior mesenteric or splenic vein. The main portal vein passes behind the duodenum, along the free border of the lesser omentum. It is typically located behind the proper hepatic artery and the common bile duct within the hepatoduodenal ligament.
At the hilum, the main portal vein divides into two branches - the right (larger) and left (smaller) portal veins. The left portal vein flows towards the umbilical fissure and gives off branches to segments 2, 3, 4 and 1. The right portal vein is short because it divides into two branches - anterior and posterior - after entering the liver. The right anterior branch supplies segments 5 and 8. Very rarely, it can also supply segment 1. The right posterior branch supplies segments 6 and 7.
Venous drainage
The venous drainage of the liver is provided by the hepatic venous system that drains the venous blood from the liver to the inferior vena cava. It consists of three major and multiple minor hepatic veins. The three major hepatic veins are located between the four liver sectors, and these are the right, middle and left hepatic veins. They collect venous blood from both surfaces of the liver and drain directly into the inferior vena cava. The right hepatic vein is found in the right portal fissure between the right anterior (medial) and posterior (lateral) sectors. It contributes to the venous drainage of segments 6 and 7 and partially segments 5 and 8.
The middle hepatic vein is located in the main portal fissures between the right and left functional lobes of the liver. It typically merges with the left hepatic vein. The middle hepatic vein drains segments 4, 5 and 8. The left hepatic vein lies in the left portal fissure between the left medial and left lateral sectors. It drains segments 2, 3 and sometimes 4. Segment 1 is drained by numerous small hepatic veins that usually flow directly into the inferior vena cava.
Lymphatic drainage
The lymph originating in the liver is usually a product of hepatic sinusoids. Overall, the liver is supplied by two lymphatic drainage systems - deep (portal and sublobular) and superficial (capsular).
The deep hepatic lymph vessels surround the portal triads between the lobules and follow the hepatic portal veins. Merging and forming larger vessels, they mostly drain into hepatic lymph nodes located at the porta hepatis, which further drain into coeliac lymph nodes. The lymph from the coeliac lymph nodes is carried next to the thoracic duct. Some lymph vessels drain to inferior diaphragmatic and phrenic lymph nodes.
The superficial hepatic lymph vessels lie along the surface of the liver. They can drain into various lymph nodes - the ones located along the inferior vena cava, next to the cardia of the stomach, at the porta hepatis or in the coeliac region. Some lymphatics can pass directly into the thoracic duct.
Innervation of liver
The innervation of the liver occurs through the sympathetic and parasympathetic nerve fibers. The parasympathetic innervation happens via the anterior and posterior vagal trunks of the vagus nerve (CN X). The sympathetic innervation comes from the greater splanchnic nerves that originate in the thoracic segments T5/6 to T9 of the spinal cord. They synapse at the coeliac ganglia and then give off postganglionic fibers.
The nerves from the right and left coeliac ganglia and the left vagus nerve form the anterior hepatic plexus. It lies along the course of the hepatic artery. In contrast, the right coeliac ganglion and the right vagus nerve form the posterior hepatic plexus. It runs posterior to the portal vein and bile duct. The fibers of the united hepatic plexus enter the liver through the porta hepatis and reach hepatocytes, running along the vessels of the portal triads.
Liver histology
The structural organization of the liver consists of parenchyma and stroma. Parenchyma is the inner component represented by a network of liver epithelial cells, while stroma surrounds it and consists of connective tissue and blood vessels. The epithelial cells of the liver are called hepatocytes. A hepatocyte is the smallest functional and cellular unit of the liver, providing secretory, metabolic and endocrine functions. Hepatocytes secrete bile, and therefore the liver is considered an exocrine gland. The hepatocytes are organized into many plates (or cords as seen in 2-D sections) containing only one layer of cells. These plates are separated by venous sinusoids anastomosing with each other and perisinusoidal spaces (spaces of Disse) located between hepatocytes and sinusoids. Since there is no basement membrane (basal lamina), the endothelial cells of the sinusoids act as a dynamic blood filter.
Structural organization of liver
A lobule is the structural (anatomical) unit of the liver. Classically, the anatomic model shows it as a hexagonal-shaped arrangement of hepatocyte plates. There are no distinct boundaries between lobules in real life, and the connective tissue is dispersed. In the center of each lobule is a central vein, a tributary of the hepatic vein. Sinusoids and hepatocyte plates radiate from the central vein to the periphery of the lobule (to portal triads).
Each lobule is separated by connective tissue that forms septae. Within the septae, at the vertices of the hexagon, the so-called portal triads are found. A portal triad contains a branch of the portal vein (portal venule), a branch of the hepatic artery (hepatic arteriole) and a bile ductule. Blood from the portal vein via sinusoids drains into the central vein that further carries venous blood to the hepatic veins via the interlobular veins. The bile flows in the opposite direction. From the hepatocytes, it flows into the network of small bile channels called canaliculi. These channels run between the hepatic plates and carry the bile to the interlobular bile ducts located within the portal triad.
Functional organization of liver
It is sometimes easier to consider the organization of the liver from a functional rather than a structural point of view. Functionally, the primary unit of the liver is an acinus. The acinus is an irregular-shaped ellipsoid mass containing hepatocytes. It is a part of the hepatic lobule between two adjacent central veins. The central part of the acinus is the connective tissue septa with the terminal branches of the hepatic arteriole and portal venules.
Each half of an acinus can be divided into three zones based on the distance from the portal blood vessels and oxygen gradient:
- Peripheral or periportal zone (zone 1) - it is the closest zone to the blood vessels and arterioles, therefore, receives the highest amount of oxygen;
- Intermediate zone (zone 2) - situated between zones 1 and 3;
- Pericentral or centrilobular zone (zone 3) - located near the central vein, receives the least amount of oxygen.
The arterial blood from the terminal hepatic arterioles can directly flow into the sinusoids or reach them via the hepatic portal venules. Therefore, the sinusoids contain mixed-blood - venous and arterial. The central veins (intralobular veins) of neighboring lobules merge and form interlobular veins. The interlobular veins form hepatic veins that drain into the inferior vena cava.
Liver cells
Hepatocytes compose around 70% of the hepatic cell population and around 70-80% of the total hepatic mass. Besides hepatocytes, the liver contains many other cells. The remaining hepatic cells include:
- Hepatic stellate cells (Ito cells)
- Liver sinusoidal endothelial cells
- Stellate sinusoidal macrophages (Kupffer cells)
- Epithelial cells of the biliary tree (cholangiocytes)
The hepatic stellate cells (Ito cells) lie between the sinusoids (sinusoidal endothelial cells) and the hepatocyte plates in the perisinusoidal spaces. The Ito cells are also known as fat-storing cells as they contain multiple inclusions of retinoids (derivatives of fat-soluble vitamin A) in their cytoplasm. Also, stellate cells secrete collagen fibers, laminin and produce growth factors responsible for the regeneration of the liver. These cells are a major component of the fibrosis process in the liver. During liver damage, they replace injured hepatocytes with collagen fibers. This process can progress into cirrhosis if the damage to the liver continues.
The liver sinusoidal endothelial cells (LSEC) are endothelial cells that line the inner surfaces of sinusoids. Because the basement membrane is absent and LSEC are fenestrated, these cells allow direct communication between the blood and hepatocytes. The stellate sinusoidal macrophages (Kupffer cells) derive from the monocytes circulating in the bloodstream. The Kupffer cells are mainly found on the endothelial surfaces of the sinusoids. The amount of these cells increases near the portal triads. Like all macrophages, these cells are responsible for the immune defense of the liver.
The cholangiocytes are epithelial cells that line the intrahepatic and extrahepatic bile ducts of the biliary tree. These cells modulate bile composition and modify the primary bile produced by hepatocytes. This entire modification process is regulated by various hormones, peptides, bile acids and other molecules.
Liver functions
The liver is a multifunctional organ providing essential functions vital for the entire human body. The broad range of these functions is discussed further.
- The liver is the central organ responsible for metabolic homeostasis, and it regulates the uptake, distribution and digestion of nutrients. It regulates the metabolization of these nutrients into energy products (blood glucose, lipids) and their subsequent storage.
- The liver detoxifies the blood by removing and eliminating potentially toxic substances such as drugs.
- Liver cells synthesize numerous proteins (albumins), amino acids (glutamate), enzymes (ALT) and vitamins (vitamin D).
- Some vitamins (vitamins A and B12), glycogen, minerals (iron, zinc) and other nutrients are stored in the liver.
- The liver is involved in the regulation of coagulation by producing coagulation factors, their inhibitors and many fibrinolytic system components.
- The liver produces and secretes a greenish-yellow fluid called bile. Its main functions include aiding in digestion and absorption of lipids and neutralization of gastric acid. Bile emulsifies lipids in the digestive tract and breaks down fat globules into smaller fat droplets. Many waste products such as bilirubin and cholesterol are excreted into bile and later eliminated from the body through feces.
- During the embryonic period, the fetal liver is responsible for the development of erythrocytes (red blood cells).
- Also, the liver provides immune function as it contains phagocytes called Kupffer cells that act against antigens.
Liver disorders
There is a wide variety of liver disorders. The most common hepatic disease is an inflammation of the hepatic cells called hepatitis. Although usually hepatitis is caused by viral infections (hepatitis A, B, C, D, E viruses), it may also be caused by some medical conditions (autoimmune, metabolic and genetic diseases) and substances (toxins, alcohol, drugs, certain medications).
Viral hepatitis is caused by one of five hepatotropic viruses - hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis D (HDV) and hepatitis E (HEV) viruses. The symptoms of viral hepatitis are very similar among all types. They may include jaundice (yellow discoloration of the skin and mucosa), malaise, fatigue, loss of appetite, nausea and vomiting, fever, dark urine and light-colored stool. Also, tenderness or abdominal pain in the right upper quadrant can be present if the liver becomes enlarged.
Alcoholic liver disease is one of the most common liver disorders, and together with hepatitis C, it is the leading cause of liver transplantation. Excessive alcohol consumption dramatically changes the microstructure of the liver tissue. The immune system via the Kupffer cells and inflammatory cells initiates the destruction of damaged hepatocytes. At the same time, these cells stimulate the proliferation of fibrous connective tissue. If the alcohol intake is not reduced and damage to the liver continues, alcoholic liver disease can result in chronic hepatitis, liver cirrhosis, liver failure and subsequent death.
References:
- Bibbo, M., & Wilbur, D. (2014). Comprehensive Cytopathology E-Book. Elsevier Gezondheidszorg.
- Brennan, P. P., Standring, S., & Wiseman, S. (2020). Gray’s Surgical Anatomy (1st ed.). Elsevier.
- Drake, R., Vogl, W., & Mitchell, A. (2019). Gray’s Anatomy for Students: With Student Consult Online Access (4th ed.). Elsevier.
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Townsend, C. (2021). Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice (21st ed.). Elsevier.
- Walls, R. N., Hockberger, R. S., & Gausche-Hill, M. (2022). Rosen’s Emergency Medicine: Concepts and Clinical Practice: 2-Volume Set. Elsevier.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app