- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
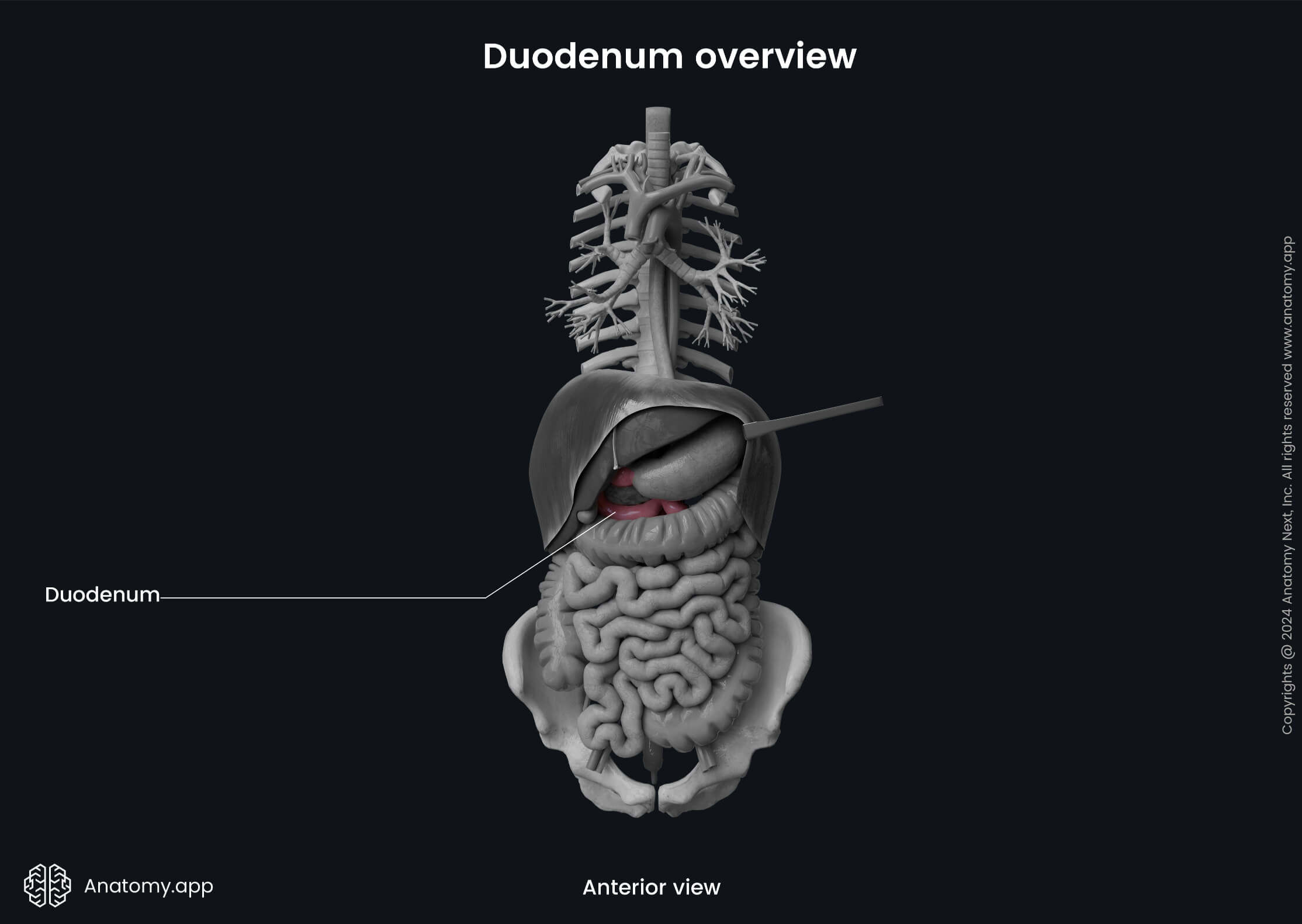
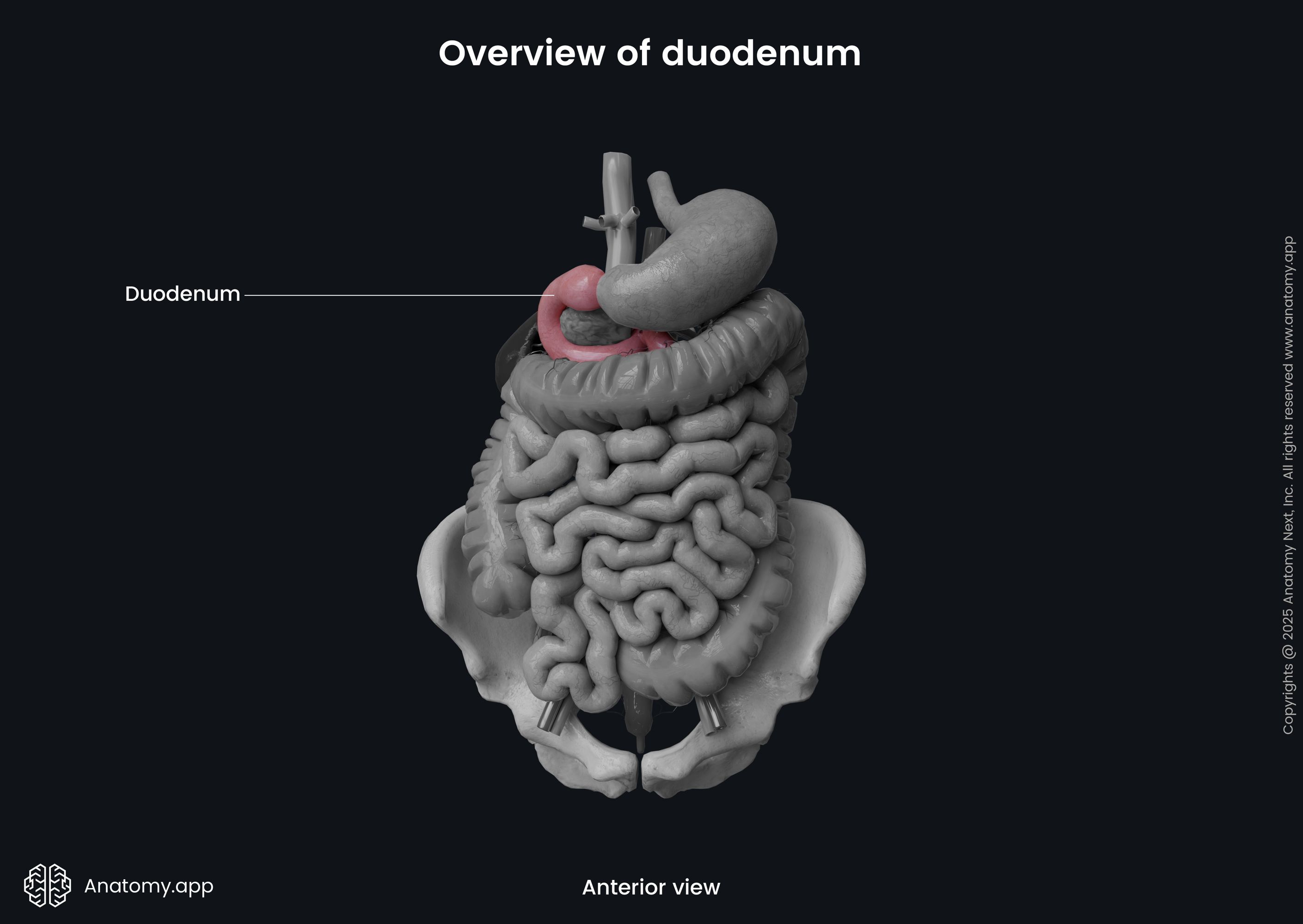
Duodenum
The duodenum (Latin: duodenum) is the first and the most proximal portion of the small intestine. It receives partially digested food from the stomach and begins intensive absorption of nutrients. The duodenum is located in the abdominal cavity inferiorly to the stomach. It is a continuation of the pyloric part of the stomach and ends by transforming into the next part of the small intestine, namely, the jejunum.
Duodenum anatomy
The Latin word duodenum means "twelve", and it comes from the Latin duodenum digitorum meaning "12 finger breadths in length". The duodenum is approximately 10 to 12 inches (25 - 30 cm) long tubular organ, the initial part of the small intestine. It is located in the abdominal cavity at the level of first to third lumbar vertebrae (L1 - L3). The shape of the duodenum resembles the letter "C" or horseshoe.
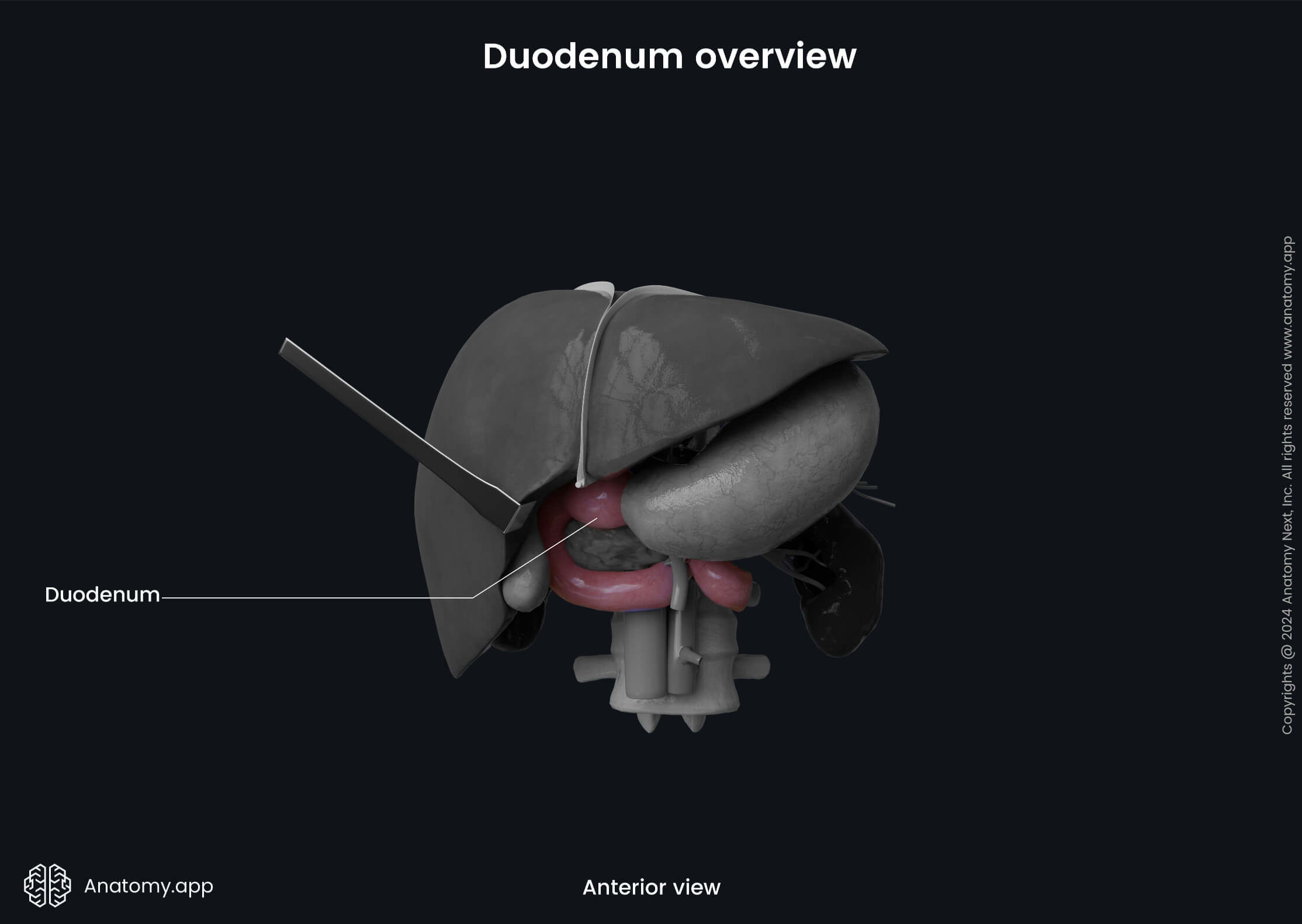
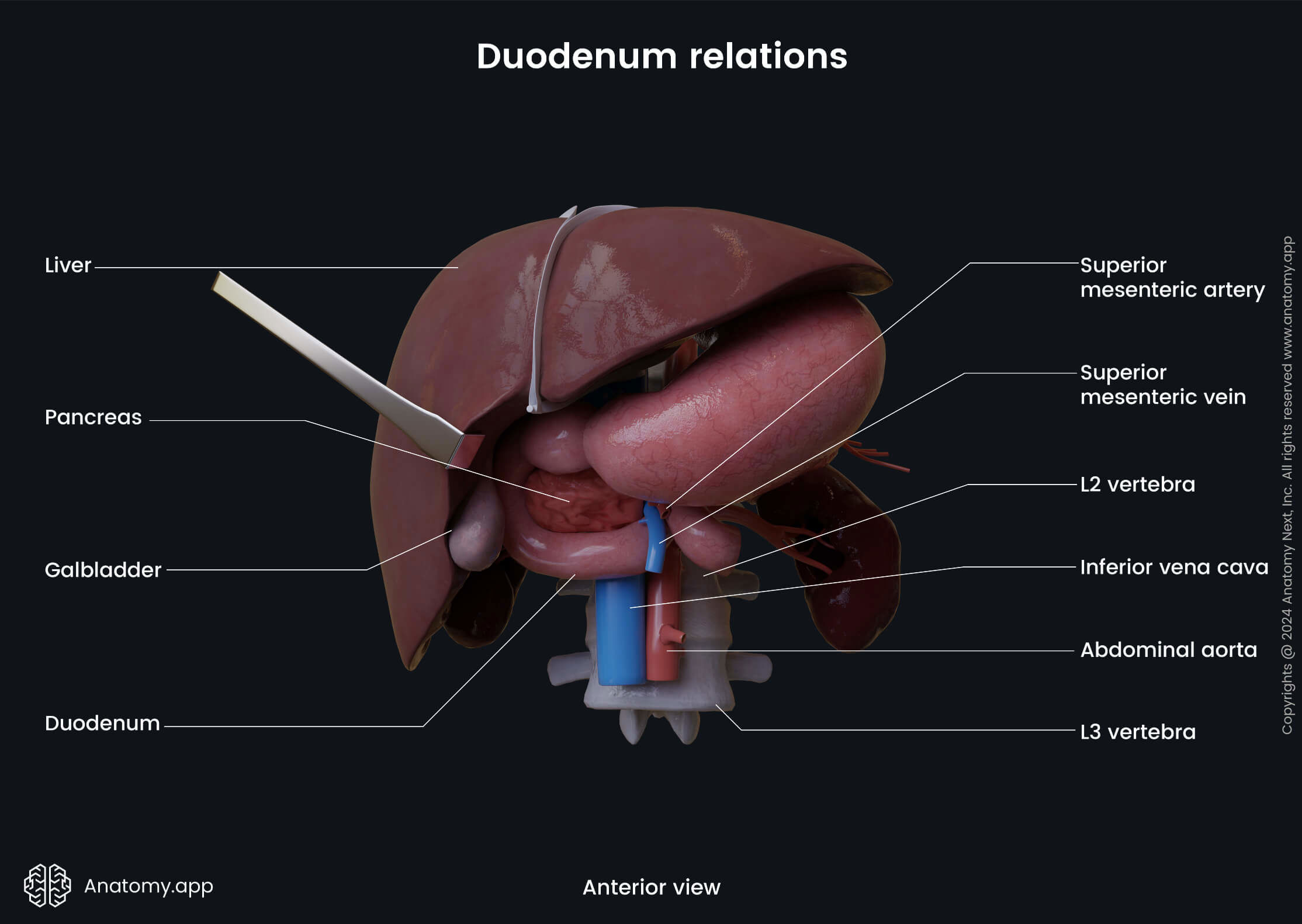
The duodenum begins from the pylorus of the stomach as its continuation. It wraps around the head of the pancreas and ends at the duodenojejunal flexure at the second lumbar vertebra (L2) level, approximately 0.8 to 1.2 inches (2 - 3 cm) from the midline. The duodenum surrounds the head of the pancreas from three sides.
Most of the duodenum is located retroperitoneally, meaning that the peritoneum covers it only from one side, and that the duodenum is situated behind it. However, the first few centimeters of the duodenum lie intraperitoneally, as they are covered posteriorly and anteriorly by the visceral layer of the peritoneum.
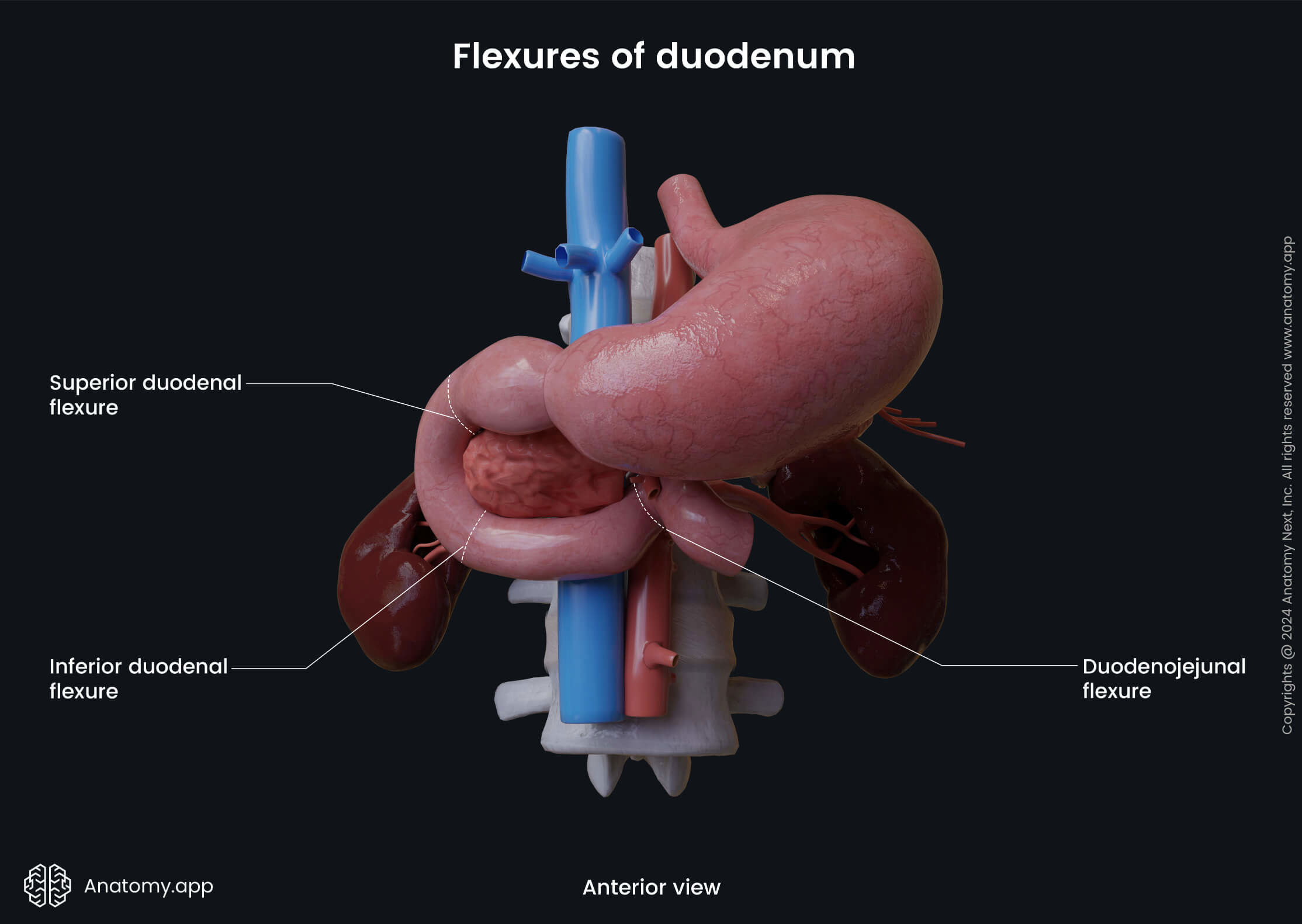
Duodenum parts and flexures
The duodenum has three flexures and four parts.
The parts of the duodenum are as follows:
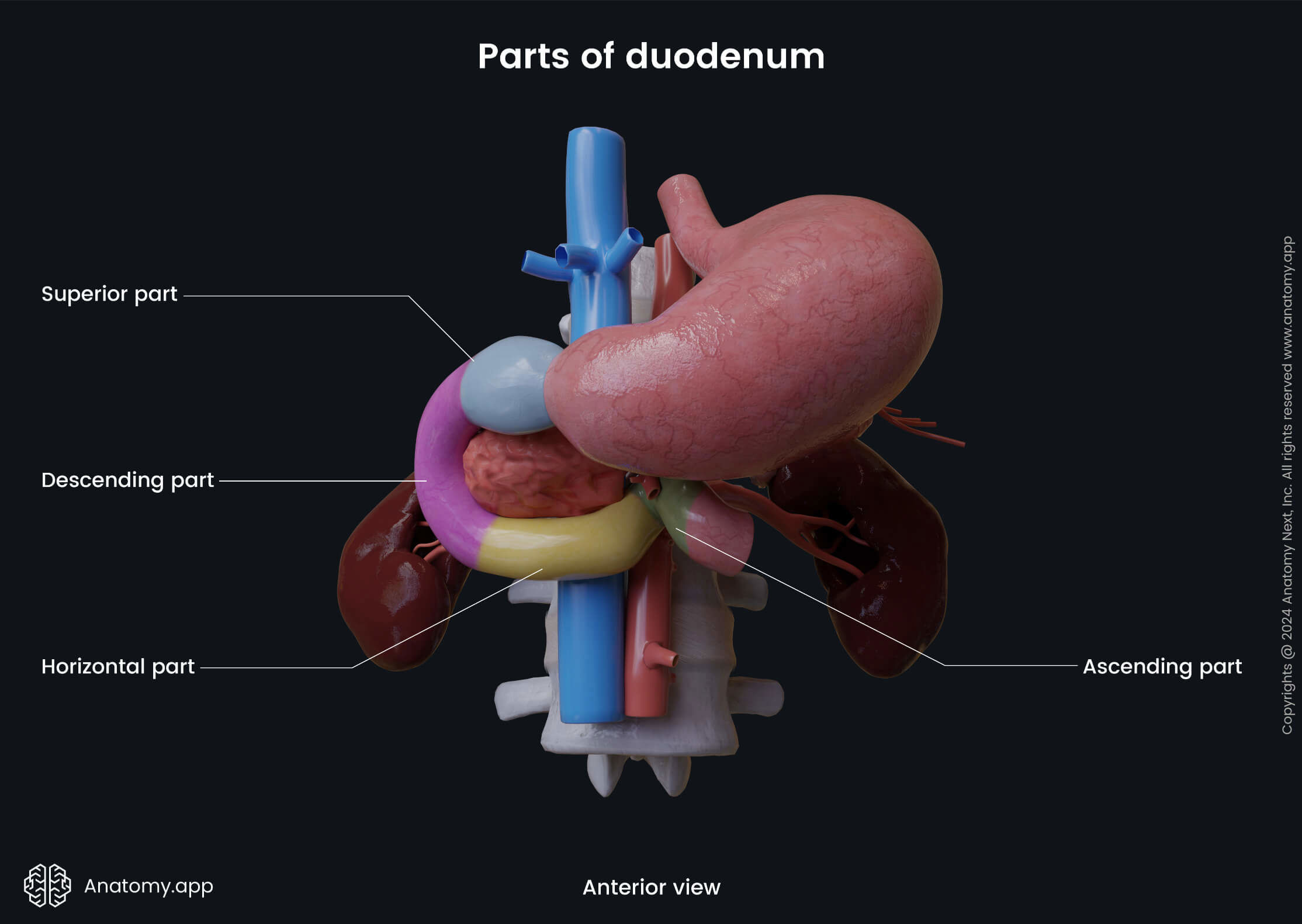
The flexures from the proximal to the distal are:
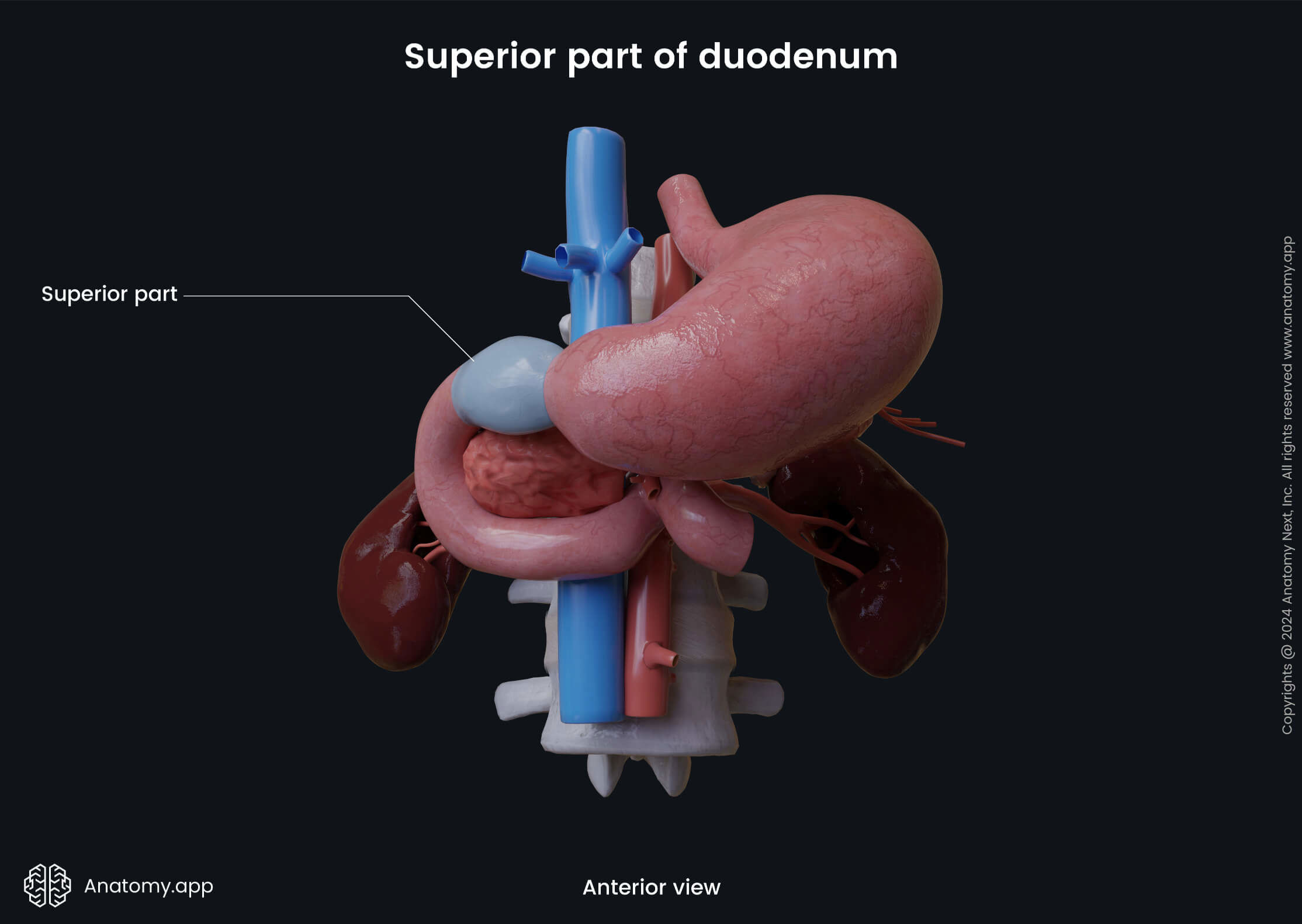
Superior part of duodenum
The superior part of the duodenum is around 2 inches (5 cm) long and it extends from the pyloric opening of the stomach to the gallbladder. It lies anterior and superior to the head of the pancreas. Posterior to it are the gastroduodenal artery, hepatic portal vein and common bile duct. Posterior to the left side of the superior part is positioned the body of the first lumbar vertebra (L1).
Clinical note: The beginning portion (around 0.7 - 1.2 inches or 2 - 3 cm) of the superior part is enlarged, and it is called the duodenal bulb or duodenal cap. The internal surface of the bulb is lined by smooth mucosa that lacs pronounced mucosal folds. Also, the duodenal bulb is the most common site where the majority of duodenal ulcers develop.
The superior part of the duodenum extends laterally, superiorly and posteriorly from the pylorus and then makes a sharp turn inferiorly at the superior duodenal flexure. This part of the duodenum also transitions from entirely intraperitoneal to a retroperitoneal position. The first 0.8 inches (2 cm) of the superior part is mobile and attached via the hepatoduodenal ligament to the liver. In contrast, the peritoneum covers only the anterior aspect of the distal 1.2 inches (3 cm) of the superior part.
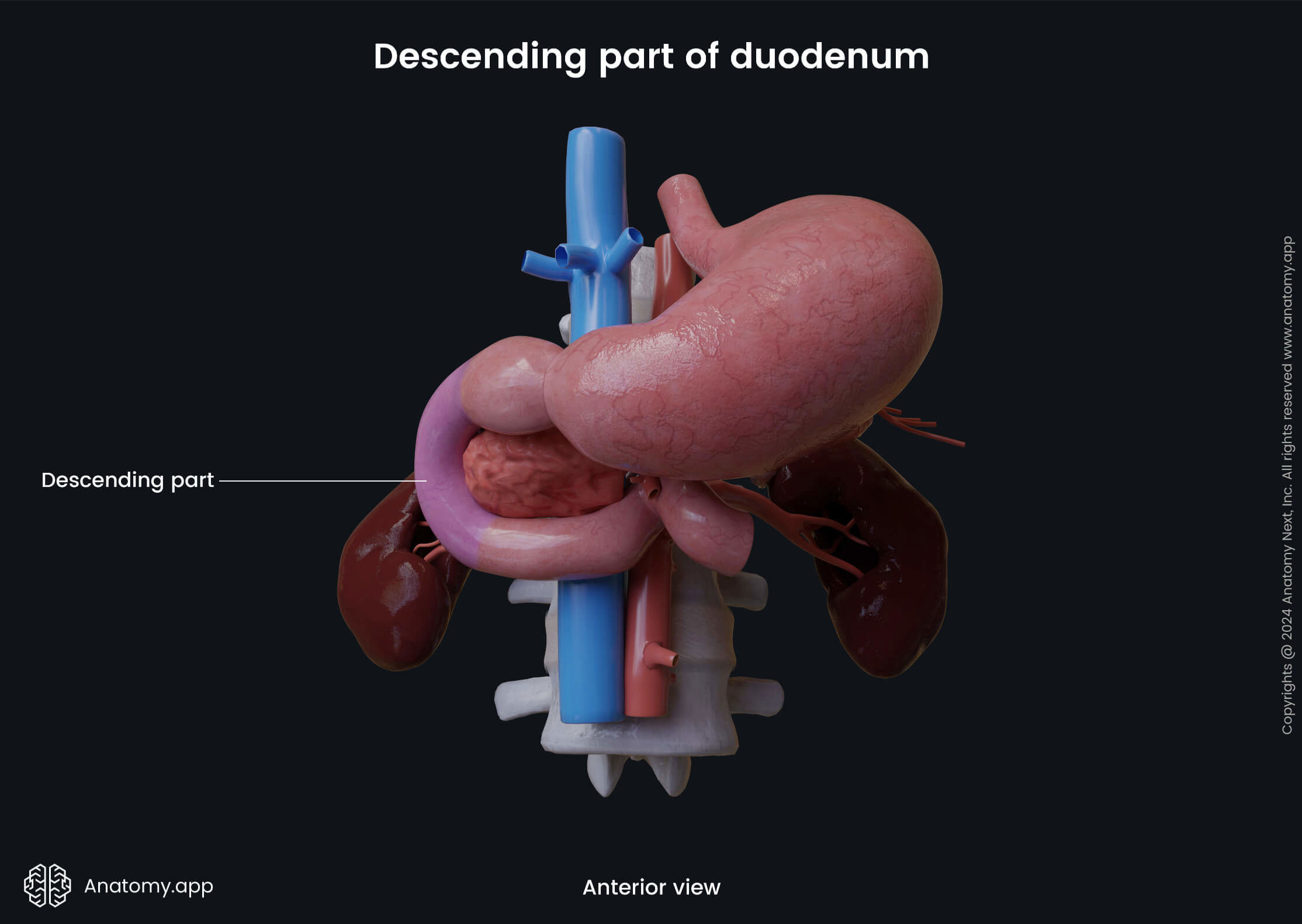
Descending part of duodenum
The descending part begins at the superior duodenal flexure and travels downward in a slightly curved manner. This part is about 2.8 - 4 inches (7 - 10 cm) long. At the third lumbar vertebra (L3) level, the descending part curves to the left side and forms the inferior duodenal flexure that further continues as the horizontal part of the duodenum.
The anterior surface of the descending duodenum is crossed by the transverse colon. Also, the right lobe of the liver, the gallbladder and coils of the small intestine lie anterior to it, while the hilum of the right kidney and right ureter are located posterior to the descending duodenum.
The head of the pancreas, the common bile duct and the main pancreatic duct are positioned medially, while lateral to the descending part of the duodenum is the ascending colon and the right colic flexure. The descending part of the duodenum has two notable anatomical landmarks - the major and minor duodenal papillae.
The major duodenal papilla (also called the papilla of Vater) is a slight mucosa elevation located within the posteromedial wall of the descending part of the duodenum. It is the common entrance site for the common bile duct and main pancreatic duct. Also, it contains the hepatopancreatic sphincter (sphincter of Oddi) that regulates the flow of bile and pancreatic secretions.
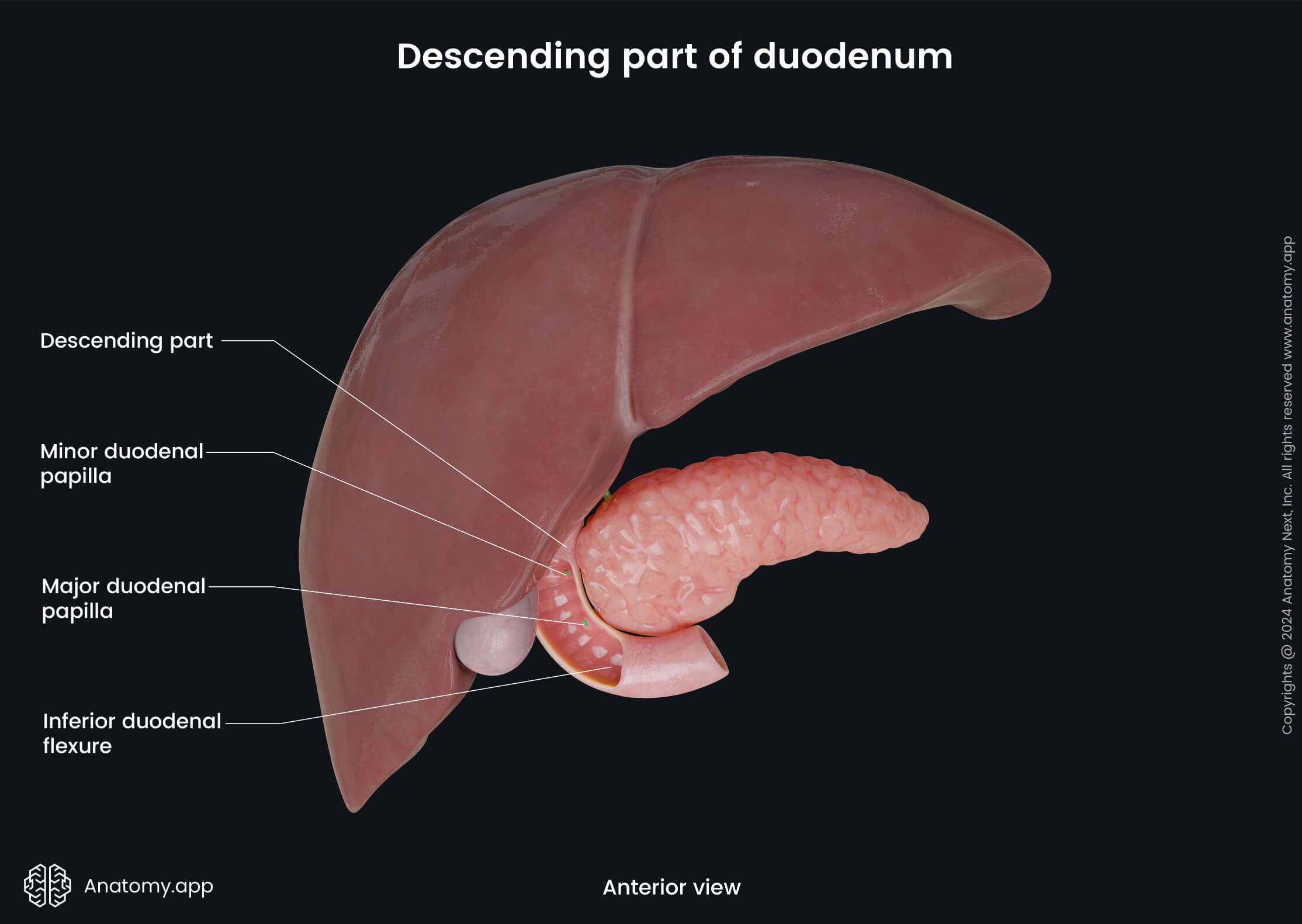
The minor duodenal papilla (also known as the papilla of Santorini) is another slight mucosal elevation within the same wall of the descending part, approximately 0.8 inches (2 cm) proximal to the major duodenal papilla. It serves as the entrance site for the accessory pancreatic duct (sometimes absent).
Horizontal part of duodenum
The horizontal part of the duodenum is the longest portion, reaching around 4 inches (10 cm) in length. It runs transversely from the right side to the left. The horizontal part starts from the inferior duodenal flexure at the right side of the third lumbar vertebra (L3) and travels to the left, crossing the inferior vena cava, abdominal aorta, and spine. When reaching the left side of the third lumbar vertebra, it further continues as the ascending part of the duodenum.
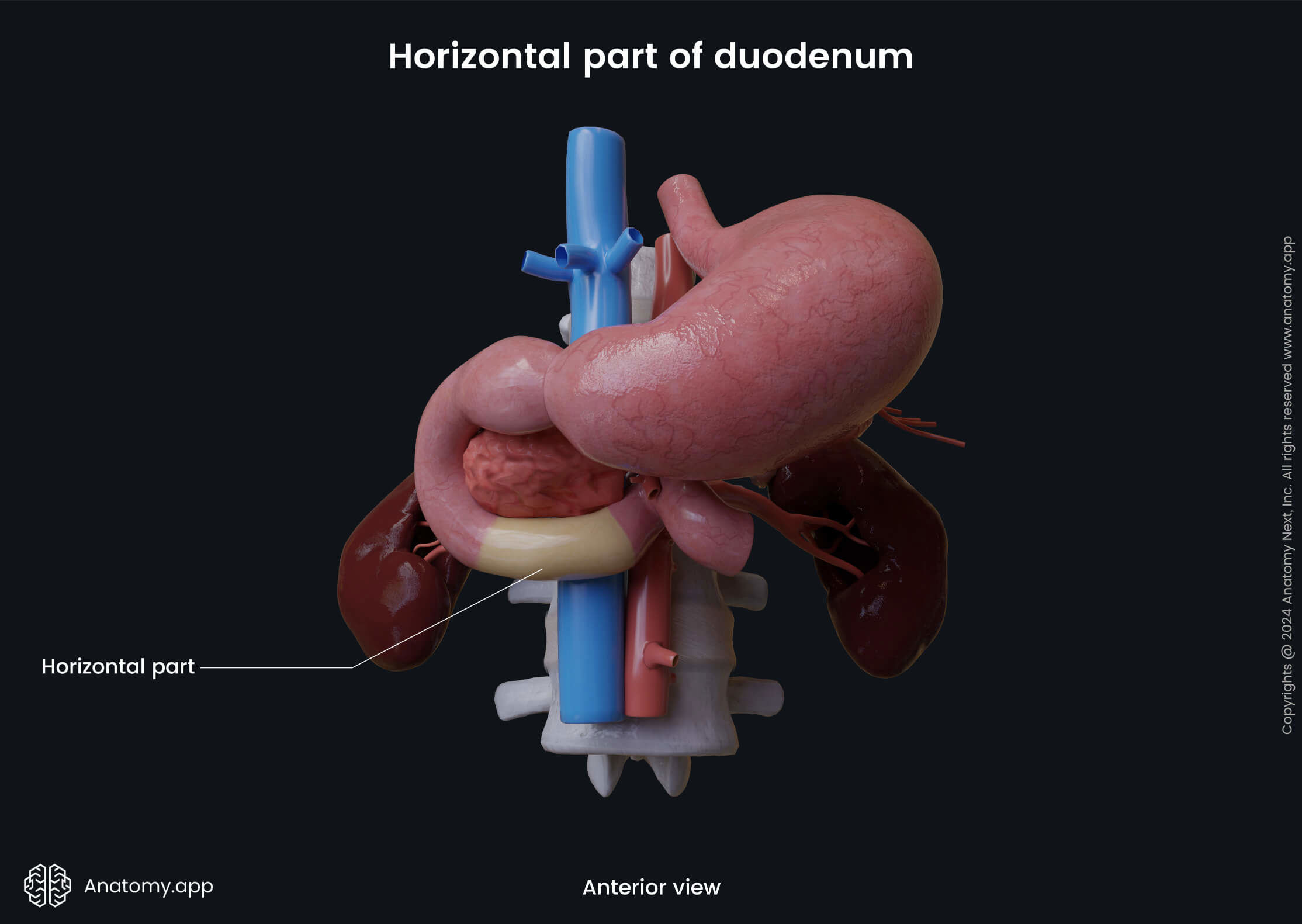
The horizontal part is located behind the superior mesenteric vessels, coils of the small intestine and root of the mesentery. While in front of it are the right ureter, right gonadal (testicular or ovarian) vessels, right psoas major muscle, third lumbar vertebra (L3), inferior vena cava, inferior mesenteric artery and abdominal aorta. The head of the pancreas lies superior to the horizontal portion, while the coils of the jejunum are positioned antero-inferiorly.
Ascending part of duodenum
The ascending part is the final portion of the duodenum, and it is up to 2 inches (5 cm) long. It starts on the left side of the abdominal aorta and third lumbar vertebra (L3) and ascends laterally to the second lumbar vertebra (L2). Further, the ascending part makes a sharp turn in an antero-inferior direction and forms the duodenojejunal flexure. The duodenojejunal flexure marks the transition site between the duodenum and jejunum.
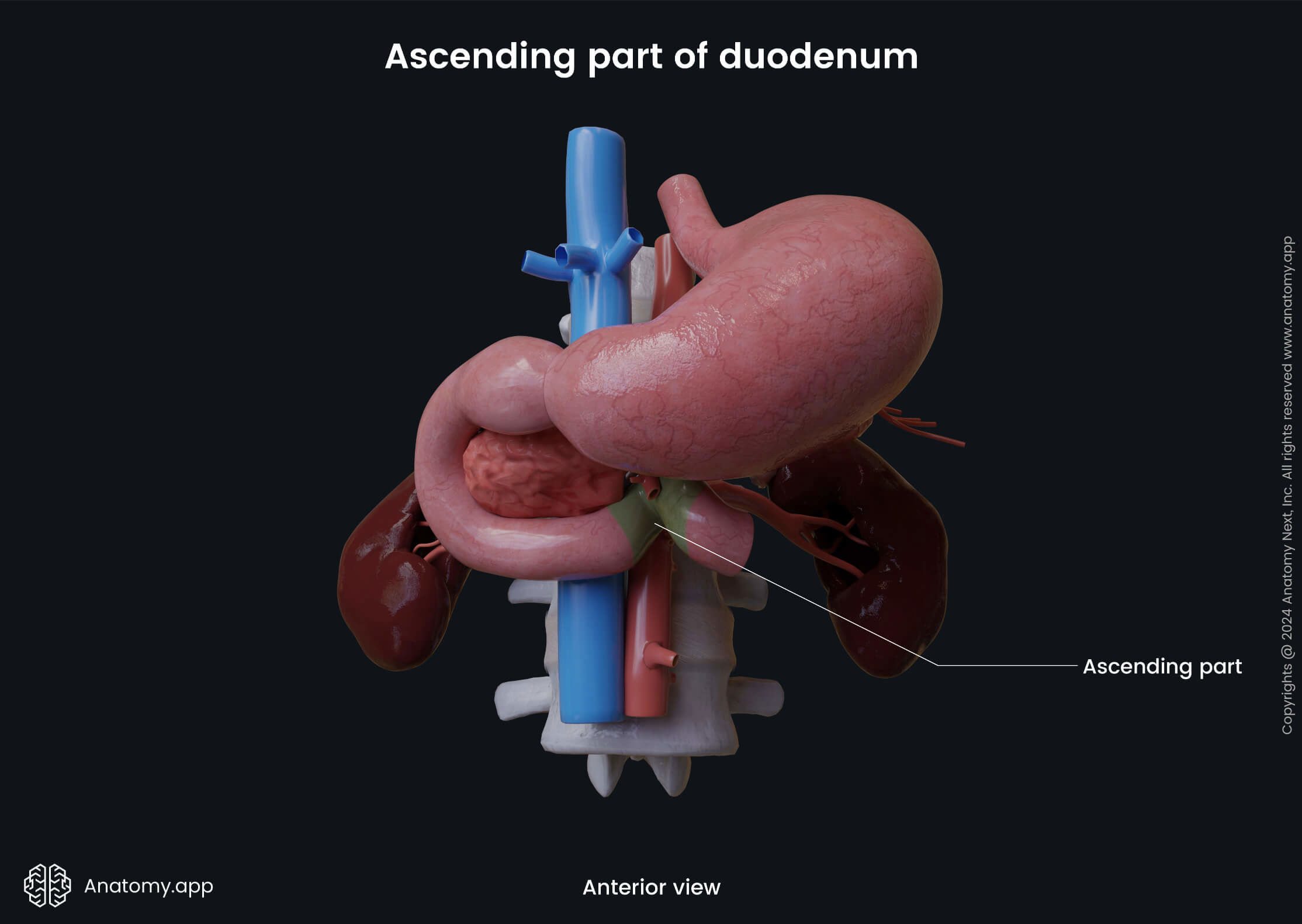
The following structures are situated posterior to the ascending part of the duodenum: left psoas major muscle, left sympathetic trunk, left renal and gonadal vessels, and inferior mesenteric vein. The transverse colon and its mesocolon are located anterior to the ascending part of the duodenum, and the body of the pancreas lies superior to it.
The ascending portion of the duodenum becomes more and more invested in the peritoneum towards the jejunum to the point that the duodenojejunal flexure is suspended from the retroperitoneum by a thin and triangular-shaped double fold of the peritoneum called the suspensory ligament of the duodenum (ligament of Treitz).
The ligament of Treitz is a fibromuscular structure, meaning that it also contains muscle fibers, and it is actually composed of two muscular parts joined by the connective tissue. Therefore, it is sometimes referred to as the suspensory muscle of the duodenum. This ligament is also used as a theoretical border between the upper and lower parts of the gastrointestinal tract.
Duodenum histology
Like in the rest of the small intestine, the wall of the duodenum is formed by four layers:
- Mucosa
- Submucosa
- Muscularis externa
- Serosa
Mucosa
The mucosa or mucosal layer faces the lumen of the duodenum and is in direct contact with its contents. It is composed of three sublayers:
- Epithelium
- Lamina propria
- Muscularis mucosae
The intestinal mucosa is lined by the simple columnar epithelium. The epithelium mainly consists of two types of cells - enterocytes and goblet cells. The enterocytes are columnar intestinal epithelial cells that primarily provide absorptive function. In contrast, the goblet cells produce and secrete mucus that helps to protect the intestine against pathogens and toxins. Also, mucus ensures lubrication and mechanical protection against intestinal contents. Besides epithelial and goblet cells, the epithelium also contains endocrine cells that produce hormones.
Beneath the epithelium is a layer called lamina propria. It is composed of loose connective tissue that supports the epithelial cells. The lamina propria of the small intestine is highly vascular, and it contains many cells, such as the fibroblasts, macrophages, plasmocytes, lymphocytes and many others to follow. Also, it includes a network of lymphoid cell aggregates and tissue called MALT (mucosa-associated lymphoid tissue).
MALT presents with lymphoid follicles containing B and T lymphocytes, as well as macrophages. The lymphoid tissue are not as pronounced in the duodenum, in comparison to other small intestine parts, as ir becomes more prominent and more in number towards the ileum.
The muscularis mucosae is the muscular layer of the mucosa formed by the smooth muscle cells, and it is situated at the base of the mucosal layer. The mucosa of the small intestine forms finger-like projections called villi. The villi are essential structures as they significantly increase the absorption area of the intestinal wall. The intestinal villi are more numerous and larger in the proximal part of the small intestine (duodenum and jejunum), while the ileum has fewer and smaller villi. The apical ends of the enterocytes are covered by other projections - microvilli. The microvilli appear as small hair-like filaments that also increase the absorption area.
Together with the submucosal layer, the mucosa forms circular mucosal folds called the circular folds (or plicae circulares, or valves of Kerckring) that encircle the lumen of the small intestine and project into it. Like the villi and microvilli, the circular folds also increase the surface area of the small intestine, thus providing the digestion and absorption of nutrients more efficiently. The circular folds are more prominent in the proximal part of the small intestine, including the duodenum, but become progressively less pronounced distally.
Another unique characteristic of the intestinal architecture is the presence of the intestinal glands (also called intestinal crypts or crypts of Lieberkühn). They are located at the bases of two adjacent villi, and they appear as mucosal pits. These glands are simple tubular glands that contain enterocytes, Goblet cells, highly specialized Paneth cells (provide an immune response and produce antibacterial substances), epithelial stem cells and neuroendocrine cells (secreting, for example, cholecystokinin). Intestinal gland cells form an alkaline fluid that dilutes chyme, thus promoting absorption.
Note: Chyme is a thick semi-fluid mass of partly digested food that is mainly mixed with gastric juice and expelled by the stomach into the duodenum.
Submucosa
The submucosa (submucosal layer) is made of loose connective tissue, and it contains blood and lymph vessels and nerve fibers. A specific characteristic of the duodenal submucosa is the presence of the submucosal glands (also called Brunner’s glands). They are branched tubular glands that secrete mucus with an alkaline pH, and the mucus neutralizes the acidic chyme coming from the stomach. Therefore, these glands are more prominent and numerous near the pylorus of the stomach and in the proximal half of the descending duodenum. Also, the submucosa of the small intestine houses the submucosal nerve plexus which is called the Meissner’s plexus.
Muscularis externa
The muscularis externa (also called muscularis propria) lies beneath the submucosa, and it consists of two distinct smooth muscle layers. The inner layer is the circular layer, and the outer is the longitudinal layer. The muscularis externa is thicker in the proximal part of the small intestine (including the duodenum), gradually becoming thinner towards its distal end. Between both layers is situated the myenteric nerve plexus - the Auerbach’s plexus.
Serosa
The serosa or serous membrane is the outermost layer of the intestinal wall and it is formed by the visceral peritoneum. The serosa is composed of two sublayers: mesothelium, which refers to the simple squamous epithelium, and supportive loose connective tissue beneath it.
Neurovascular supply of duodenum
Arterial blood supply
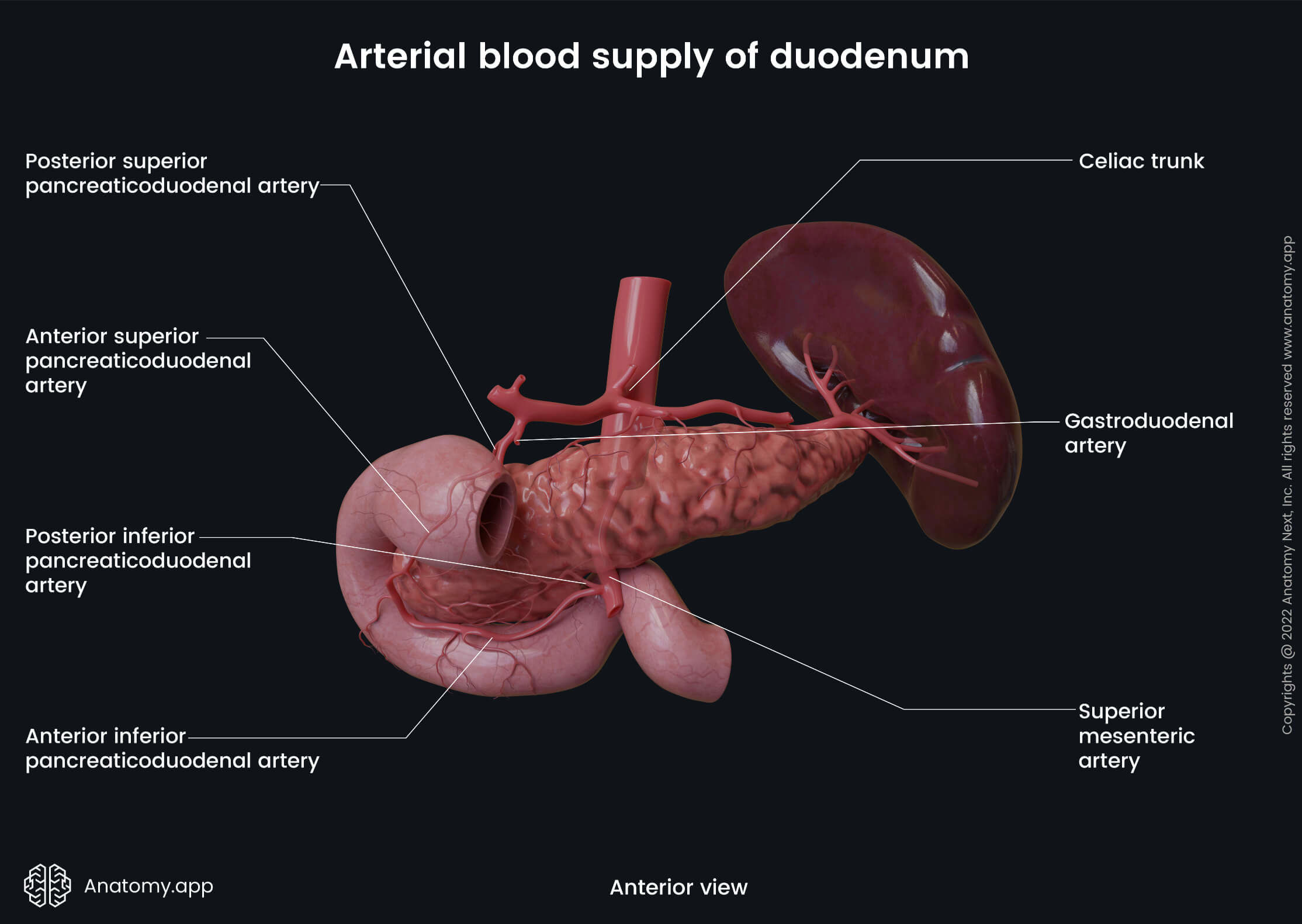
The arterial blood supply to the duodenum and the rest of the small intestine is provided by branches of the celiac trunk and the superior mesenteric artery. The superior and descending parts of the duodenum until the major duodenal papilla are supplied by branches of the celiac trunk. In contrast, the duodenum distal to the major duodenal papilla receives arterial blood from branches of the superior mesenteric artery.
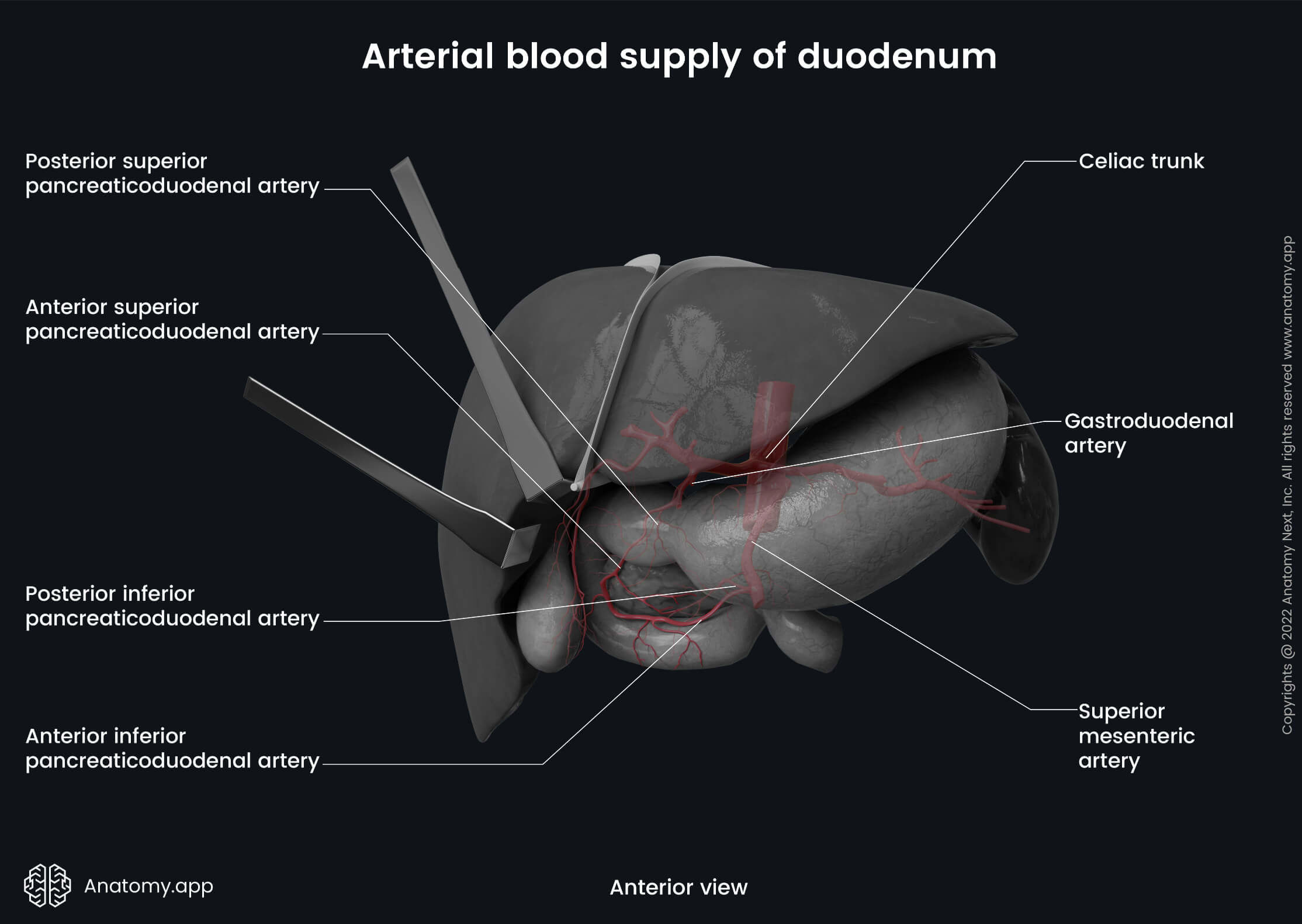
The main arterial supply to the duodenum is ensured by two anterior (superior and inferior) and two posterior (superior and inferior) pancreaticoduodenal arteries. The anterior superior and posterior superior pancreaticoduodenal arteries arise from the gastroduodenal artery (a branch of the common hepatic artery that originates from the celiac trunk), and they supply the superior and descending parts (till the major duodenal papilla) of the duodenum. The anterior inferior and posterior inferior pancreaticoduodenal arteries are branches of the superior mesenteric artery, and they supply the remaining descending part, horizontal and ascending portions of the duodenum.
Venous drainage
The venous drainage of the duodenum is provided by the portal venous system. It occurs via small duodenal veins that carry venous blood further to the superior and inferior pancreaticoduodenal veins that follow the corresponding arteries and drain into the hepatic portal vein either directly or indirectly.
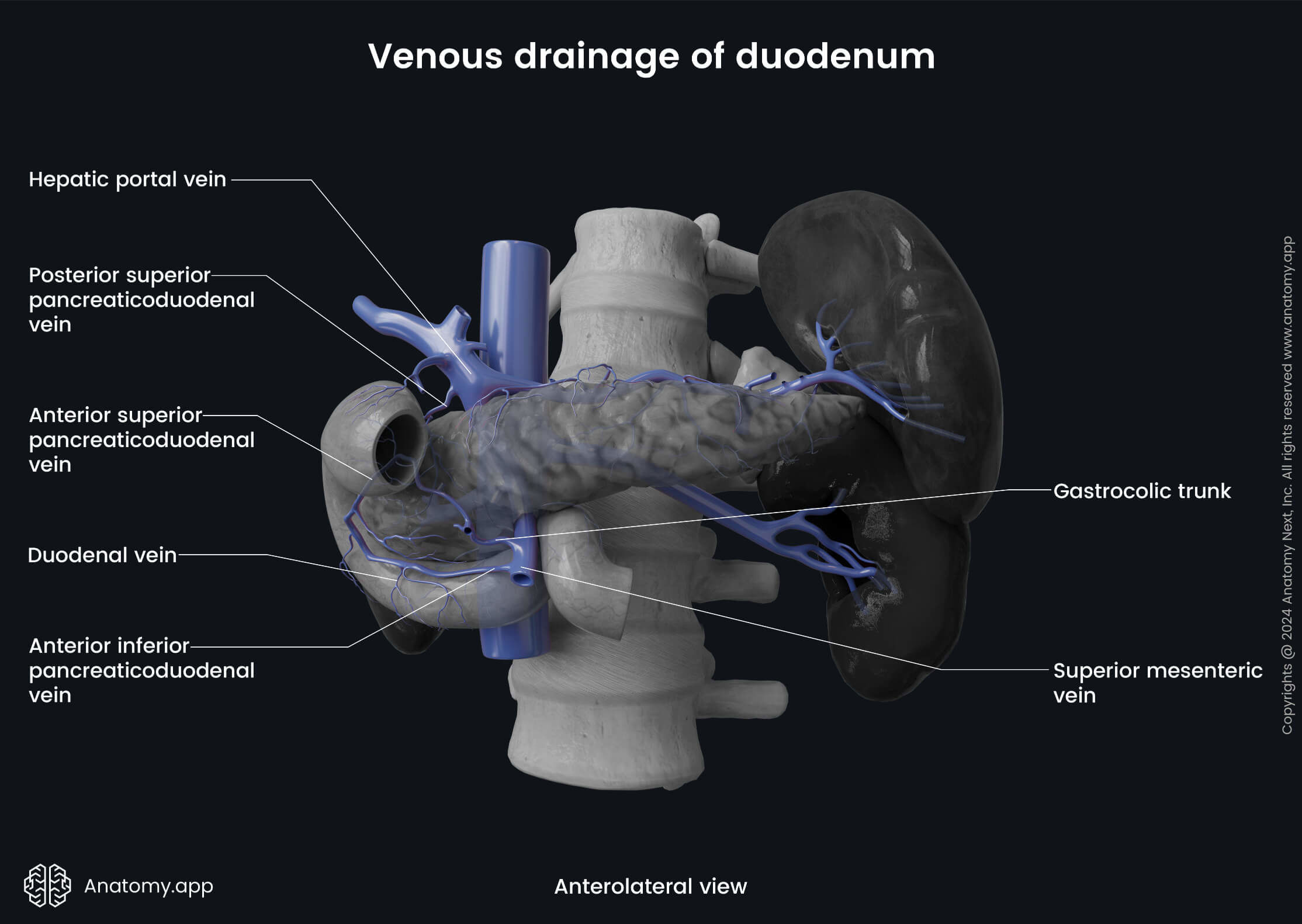
Each person has four pancreaticoduodenal veins - anterior superior pancreaticoduodenal vein, posterior superior pancreaticoduodenal vein, anterior inferior pancreaticoduodenal vein and posterior inferior pancreaticoduodenal vein. The posterior superior pancreaticoduodenal vein drains into the hepatic portal vein, while the anterior superior pancreaticoduodenal vein flows into the gastrocolic trunk or the right gastro-omental vein. The posterior and anterior inferior pancreaticoduodenal veins drain into the superior mesenteric vein or its first jejunal tributary.
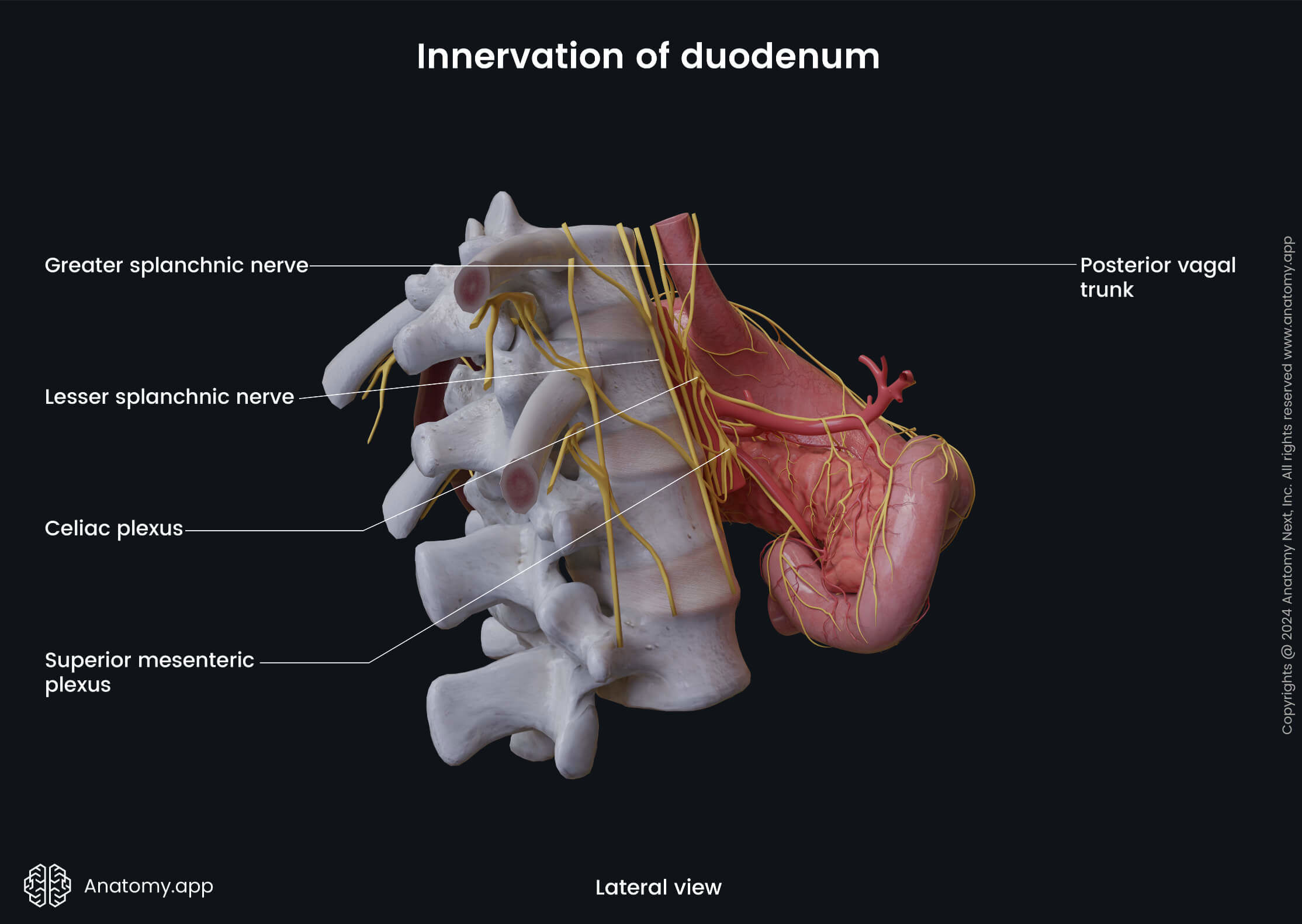
Innervation
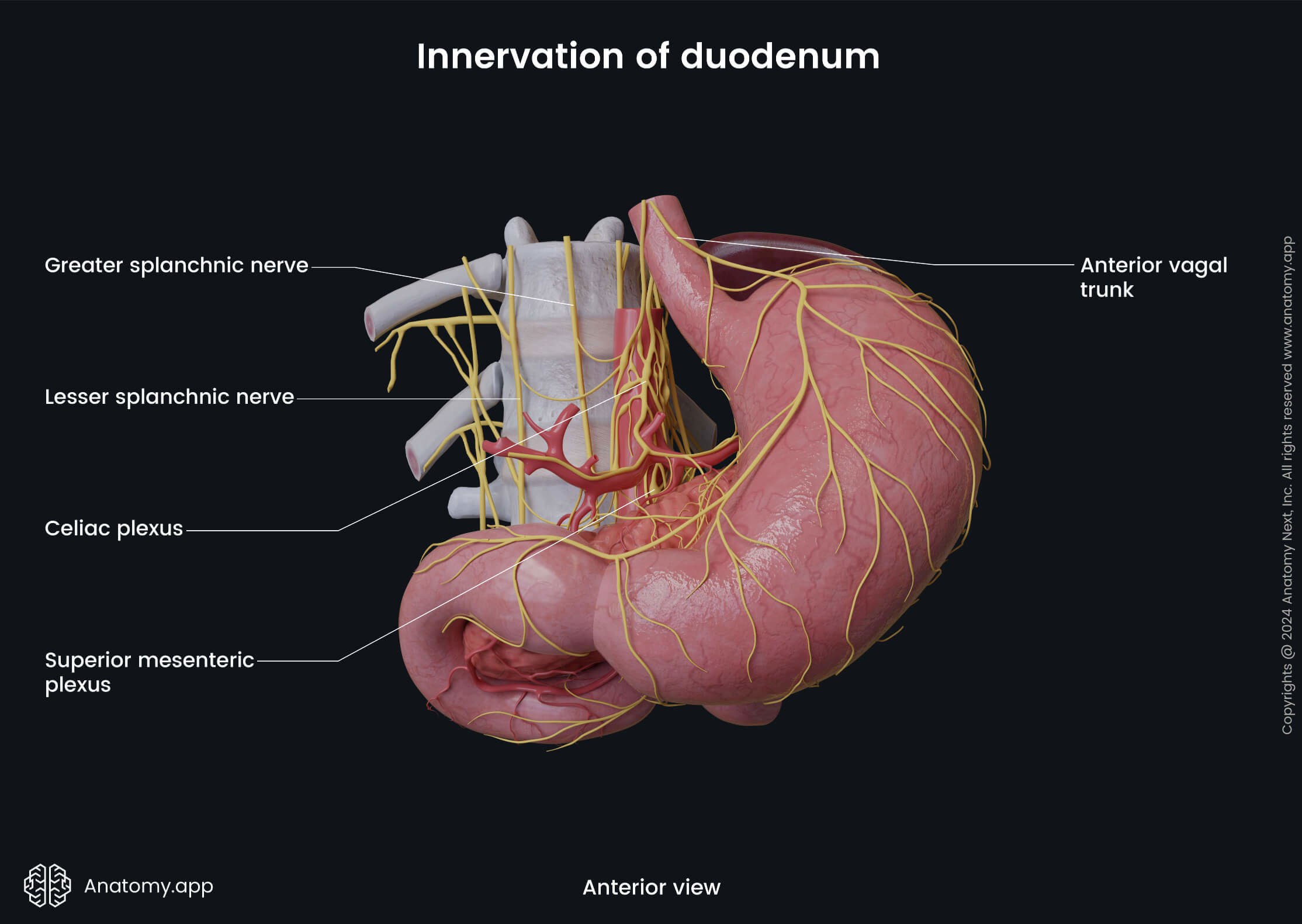
The duodenum receives sympathetic and parasympathetic innervation. The sympathetic innervation of the duodenum occurs via the greater thoracic splanchnic nerves that participate in the formation of the superior mesenteric plexus around the superior mesenteric artery and celiac plexus around the celiac trunk. The sympathetic fibers ensure vasoconstriction (narrowing of the lumen of blood vessels) of the intestinal vessels, relaxation of smooth muscle cells and inhibition of intestinal gland secretion.
The bodies of the preganglionic sympathetic neurons are located in the gray matter of the fifth to tenth thoracic segments (duodenum: T5 - T9, jejunum and ileum: T9 - T10) of the spinal cord. Axons of these neurons form the greater and lesser thoracic splanchnic nerves that travel to the celiac and superior mesenteric plexuses and synapse there with the neurons of the celiac and superior mesenteric ganglia. Postganglionic axons then travel to the small intestine via the periarterial branches and supply it.
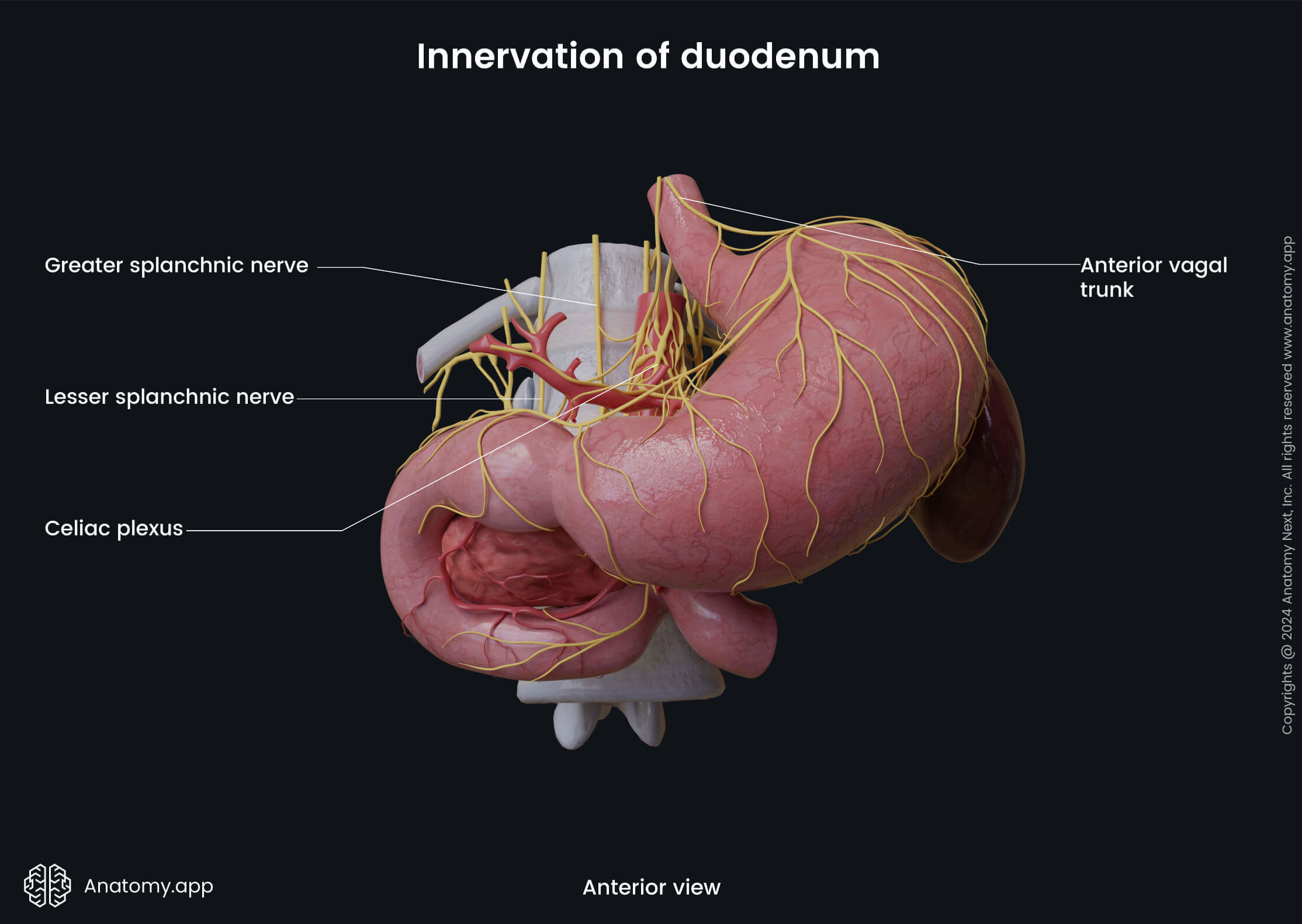
In contrast, the parasympathetic innervation of the duodenum is provided by fibers of the vagus nerve (CN X) via the anterior and posterior vagal trunks. The parasympathetic fibers stimulate intestinal gland secretion and smooth muscle cell contractions. Also, they provide vasodilation (widening of the lumen of vessels) of the intestinal blood vessels.
The nerve fibers of both systems extend throughout the entire length of the small intestine and synapse with the neurons located in the intestinal wall, forming two plexuses:
- Submucosal plexus (Meissner’s plexus) - located in the submucosal layer; contains only the parasympathetic fibers;
- Myenteric plexus (Auerbach’s plexus) - positioned in the muscularis externa between both its layers; contains parasympathetic and sympathetic nerve fibers.
Lymphatic drainage
The lymph collected from the duodenum drains to the pancreaticoduodenal lymph nodes located along the superior and inferior pancreaticoduodenal arteries, pyloric lymph nodes found around the pylorus of the stomach, superior mesenteric lymph nodes situated along the superior mesenteric artery and celiac lymph nodes along the celiac trunk.
Duodenum functions
The main functions of the duodenum include nutrient breakdown, the absorption of the nutrients (proteins, fats, carbohydrates, vitamins and minerals) and water from partially digested food, secretion of hormones and intestinal juice, and also immune responses.
The intestinal epithelial cells are also responsible for the absorption of electrolytes and water. The majority of the water absorption occurs in the proximal small intestine, while the remaining water is absorbed by the large intestine. The duodenum also helps to neutralize the gastric juice as its glands produce alkaline mucus.
The gastrointestinal tract organs produce numerous enzymes necessary for nutrient breakdown which starts in the duodenum and mostly happens in the small intestine. The digestive enzymes are mainly secreted by the pancreas, and they are released in the small intestine via the main pancreatic duct that opens in the descending part of the duodenum. The chyme mixes with digestive juices in the duodenum.
Proteins are broken down into amino acids, and complex carbohydrates break down into monosaccharides. And finally, fats break down into fatty acids and glycerol. Before the breakdown, fats are emulsified by the bile that reaches the duodenum via the vessels of the biliary tree. Minerals, such as calcium, iron, magnesium and phosphorus, are absorbed mainly in the duodenum and proximal jejunum.
The duodenum also helps to regulate and intensify intestinal motility - movements provided by the muscle fibers within the small intestine wall. These muscle contractions transit intestinal content towards the large intestine. The duodenum also participates in immune responses, as the lymphatic tissue aggregates and Paneth cells protect the intestines against antigenes.
References:
- Drake, R., Vogl, W., & Mitchell, A. (2019). Gray’s Anatomy for Students: With Student Consult Online Access (4th ed.). Elsevier.
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Moore, K.L., Dalley, A.F., Agur, A.M. (2018). Clinically Oriented Anatomy, 8th Edition, Lippincott Williams & Wilkins.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app