- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
Bronchi
Bronchi (plural in Latin: bronchi, singular: bronchus) are flexible air tubes located inside the thoracic cage. The bronchi generally are conducting airways that contain cartilages. They belong to the lower airways and are part of the tracheobronchial tree that connects the trachea to the lungs.
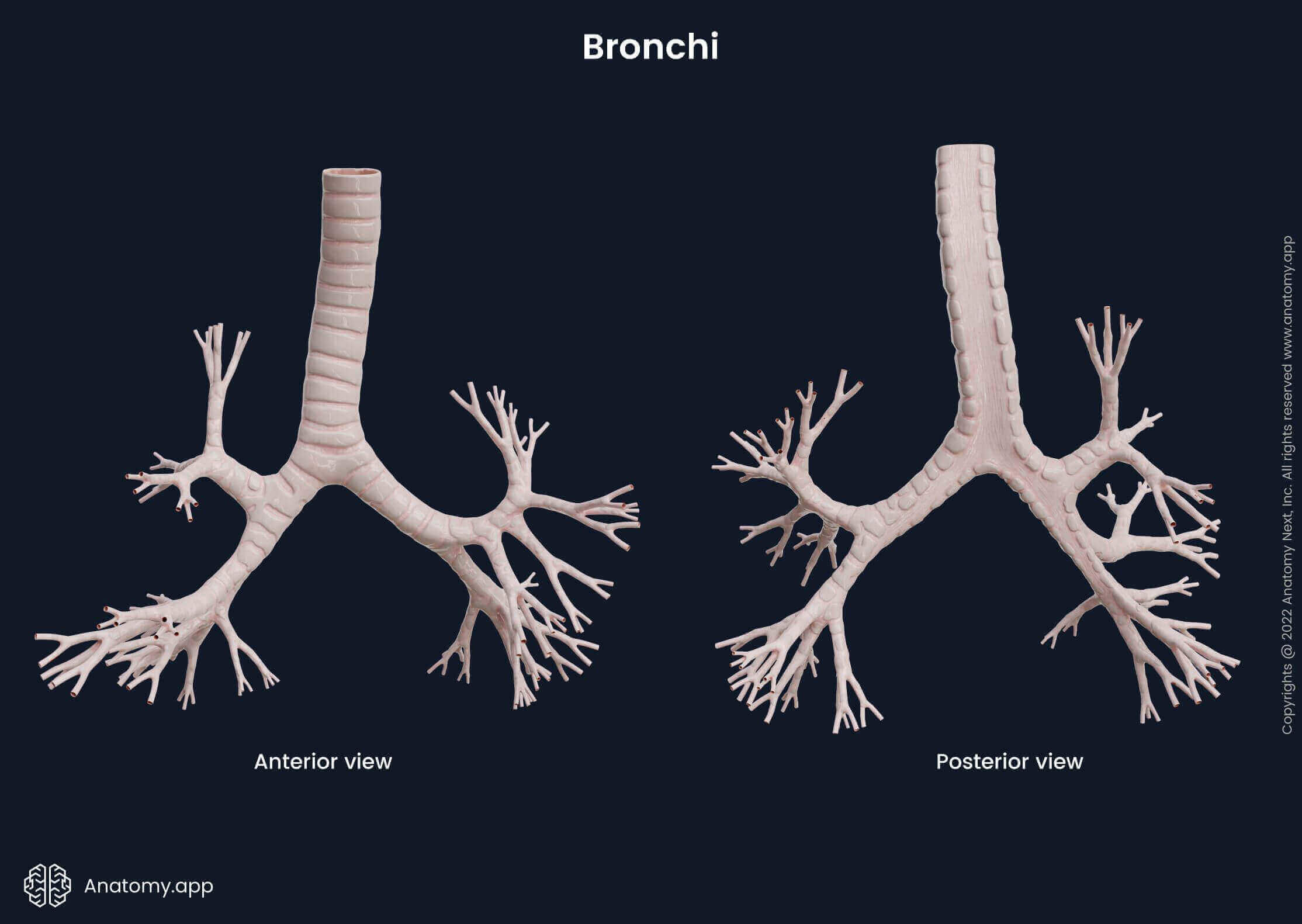
The lower airways divide into branches that become progressively smaller in diameter and multiply in number, resembling a tree with branches. Therefore, they are collectively referred to as the tracheobronchial tree. Overall, there are around 16 generations of bronchi and bronchioles in the human respiratory tract. The tracheobronchial tree is divided more or less symmetrically in both lungs.
| Overview of bronchi | |||
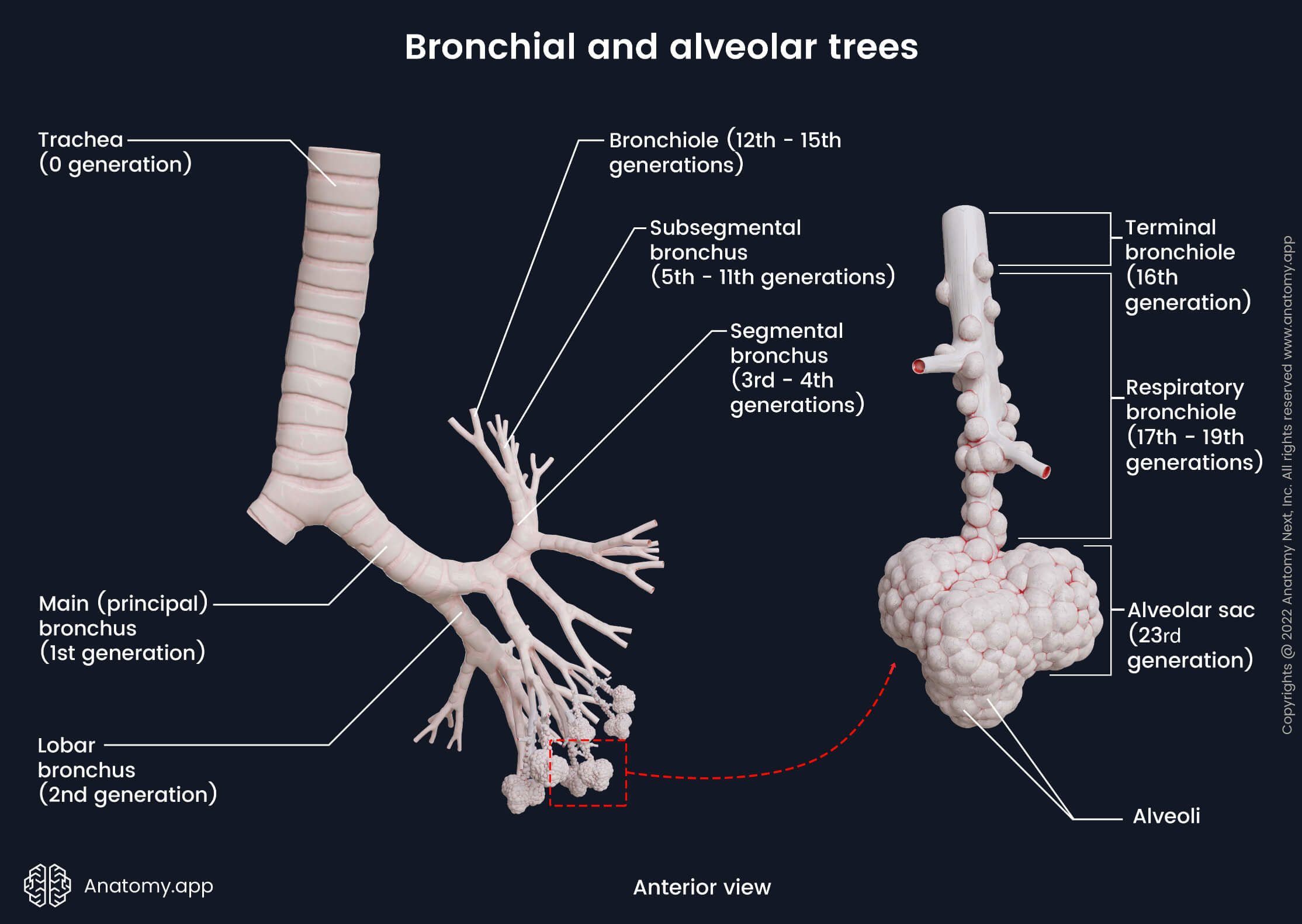
| Branching patterns of tracheobronchial tree | alveolar tree | Trachea -> main (principal) bronchi -> lobar bronchi -> segmental bronchi -> subsegmental bronchi -> bronchioles -> terminal bronchioles | -> respiratory bronchioles -> alveolar ducts -> alveolar sacs -> alveoli | ||
| Subdivisions of large bronchi | Right main bronchus | Superior lobar bronchus | Apical segmental bronchus |
| Anterior segmental bronchus | |||
| Posterior segmental bronchus | |||
| Middle lobar bronchus | Medial segmental bronchus | ||
| Lateral segmental bronchus | |||
| Inferior lobar bronchus | Superior segmental bronchus | ||
| Medial basal segmental bronchus | |||
| Lateral basal segmental bronchus | |||
| Anterior basal segmental bronchus | |||
| Posterior basal segmental bronchus | |||
| Left main bronchus | Superior lobar bronchus | Apicoposterior segmental bronchus | |
| Anterior segmental bronchus | |||
| Superior lingular segmental bronchus | |||
| Inferior lingular segmental bronchus | |||
| Inferior lobar bronchus | Superior segmental bronchus | ||
| Anteromedial basal segmental bronchus | |||
| Lateral basal segmental bronchus | |||
| Posterior basal segmental bronchus | |||
| Arterial blood supply | Bronchial arteries | ||
| Venous drainage | Superficial bronchial veins -> azygos vein (right side) / superior intercostal vein or accessory hemiazygos vein (left side) Deep bronchial veins -> pulmonary veins or directly into left atrium | ||
| Lymphatic drainage | Deep lymphatic plexus -> pulmonary lymph nodes -> bronchopulmonary (hilar) lymph nodes -> tracheobronchial lymph nodes -> paratracheal lymph nodes -> bronchomediastinal trunks -> thoracic duct (left side) / right lymphatic duct (right side) | ||
| Innervation | Branches of vagus nerve (CN X) and sympathetic trunk via anterior and posterior pulmonary plexuses | ||
Anatomy of bronchi
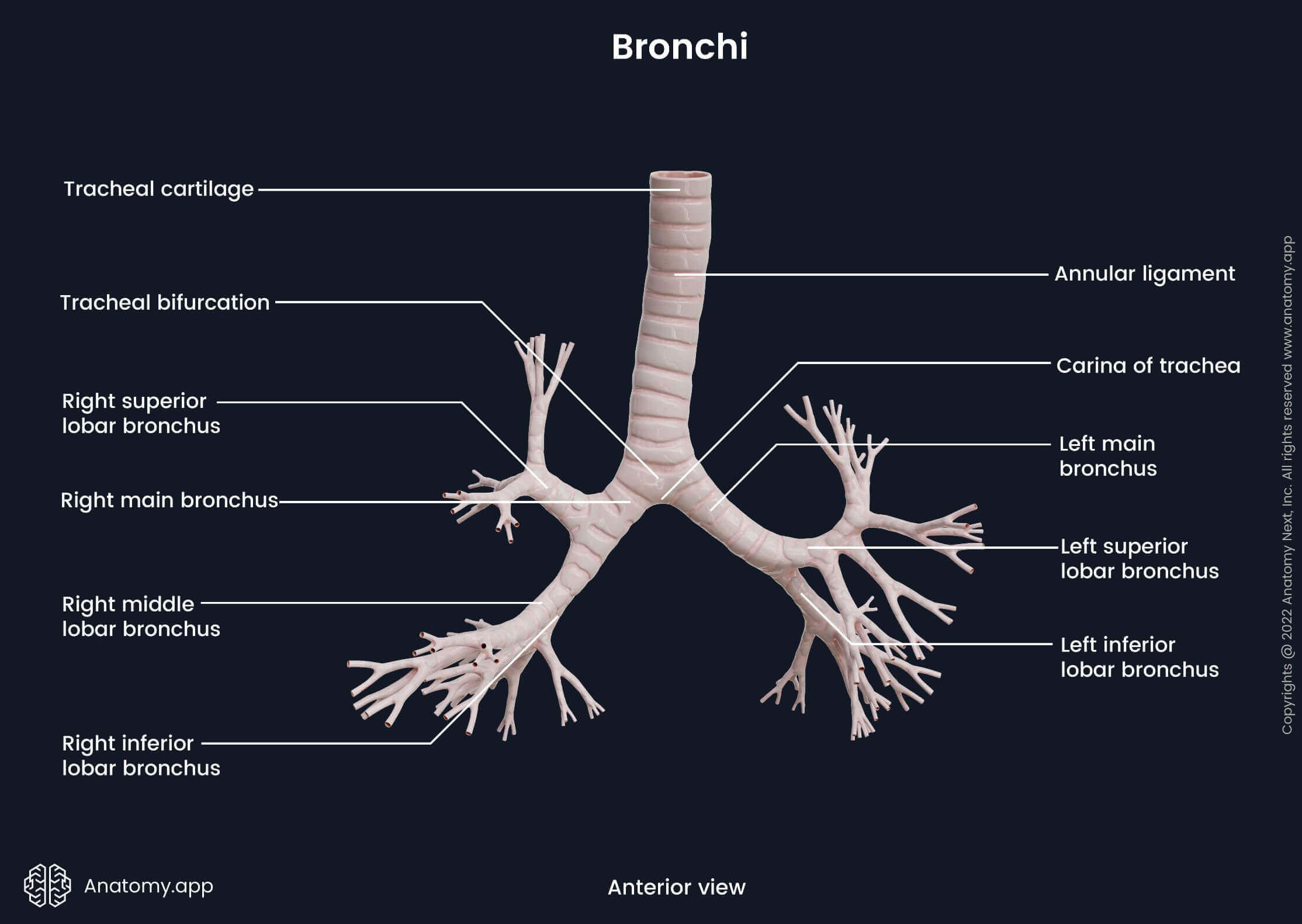
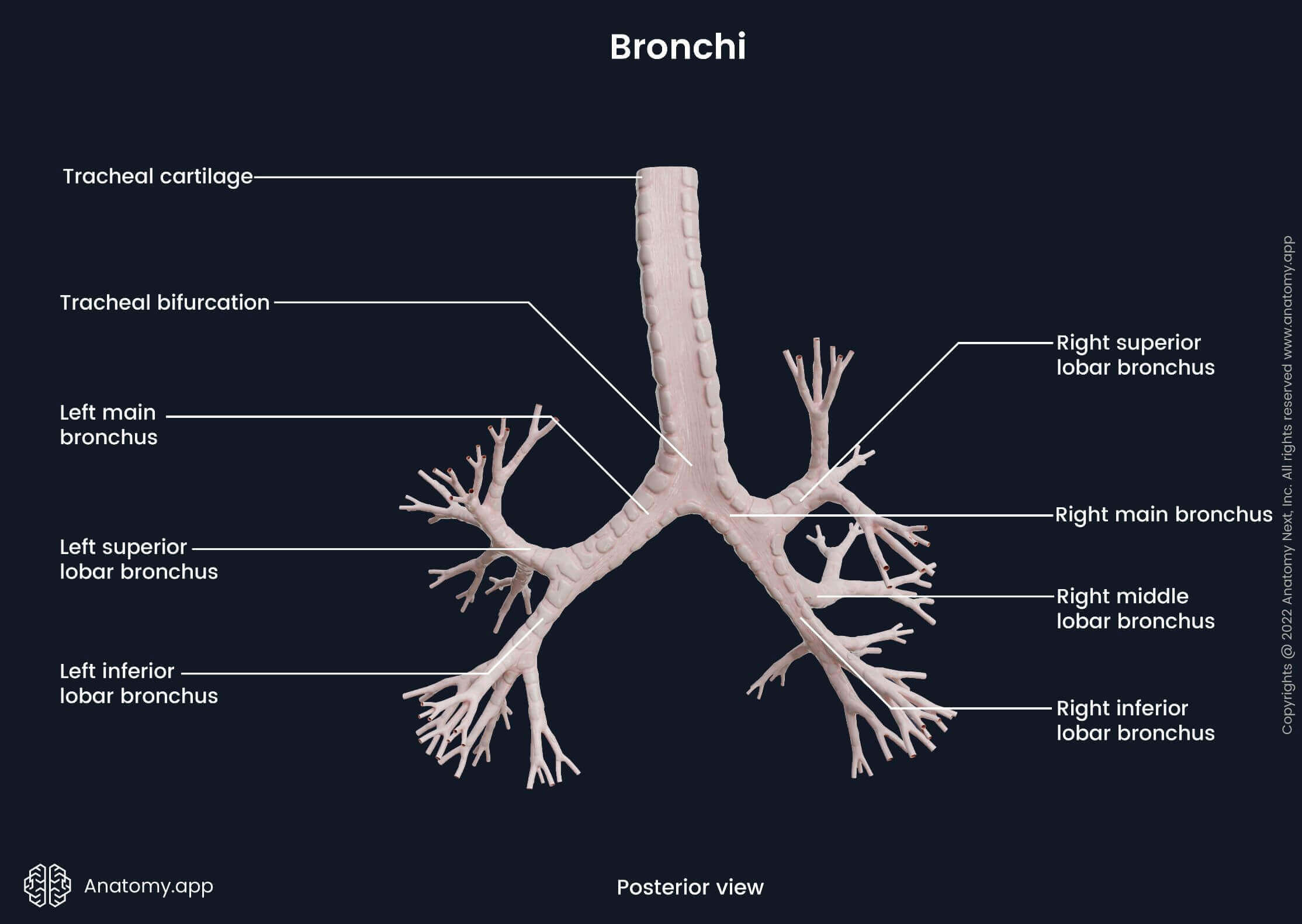
At the level of the carina, the trachea divides into two main (principal) bronchi - right and left. The tracheal carina is a ridge at the tracheal bifurcation that usually projects at the sixth thoracic vertebral body (T6) level (ranging from T4/ 5 to T7). Each main bronchus enters the lung through the hilum of the lung. The main bronchi are then divided into smaller branches - secondary and tertiary bronchi. First, the bronchi are divided into the lobar bronchi (secondary bronchi) corresponding to lobes of the lungs. The right lung has three lobes and three lobar bronchi. The left lung contains two lobes, and therefore, it has two lobar bronchi.
The lobar bronchi continue to divide further into segmental bronchi (tertiary bronchi). They are located according to the corresponding bronchopulmonary segments of each lung. A bronchopulmonary segment is a separate anatomical, physiological and surgical unit of the lungs. Each unit is separated by a layer of connective tissue that merges with the visceral pleura. Also, each bronchopulmonary segment contains a segmental bronchus and its adjacent pulmonary artery. Each lung contains ten bronchopulmonary segments. However, several segments of the left lung are sometimes classified as one segment. Therefore, the left lung occasionally has only eight bronchopulmonary segments instead of ten.
The segmental bronchi further divide into several generations of subsegmental bronchi. They become increasingly narrow, progressively loose their cartilage and divide further into bronchioles. The bronchioles are conducting airways of smaller diameters (usually ∼1 mm) and, in contrast to bronchi, their wall does not contain cartilage or submucosal glands. They are also surrounded by the connective tissue of the lungs. The bronchioles are short. They end with a part that is called the terminal bronchiole.
The tracheobronchial branching system up until the terminal bronchioles is considered non-respiratory and is known as the conducting zone. Its main function is the conduction of inhailed air, meaning, its components primarly serve as passageways for air to travel to and from the lungs. The terminal bronchioles further continue as the respiratory bronchioles. They form the transitional zone (between the conducting zone and the respiratory zone), as they can participate in gas exchange to some extent. The respiratory zone consists of the alveolar ducts and alveolar sacs containing the alveoli. The primary function of this zone is gas exchange.
Right main bronchus and its subdivisions
The right main bronchus is shorter, wider and more vertical than the left bronchus. This anatomical characteristic causes the inhaled foreign particles and bodies to enter the right bronchus more often than the left one. The right main bronchus divides into three lobar bronchi: superior, middle, and inferior.
The first branch of the right main bronchus is the superior lobar bronchus. It branches off before entering the hilum of the right lung. The superior lobar bronchus gives rise to three segmental bronchi:
- Apical segmental bronchus - continues to supply the apex of the lung;
- Posterior segmental bronchus - supplies the posteroinferior part of the superior lobe;
- Anterior segmental bronchus - supplies the rest of the superior lobe.
At the superior border of the hilus, the azygos vein curves around the superior lobar bronchus and enters the superior vena cava. The right pulmonary artery relates first to the inferior surface then to the anterior surface of the right main bronchus.
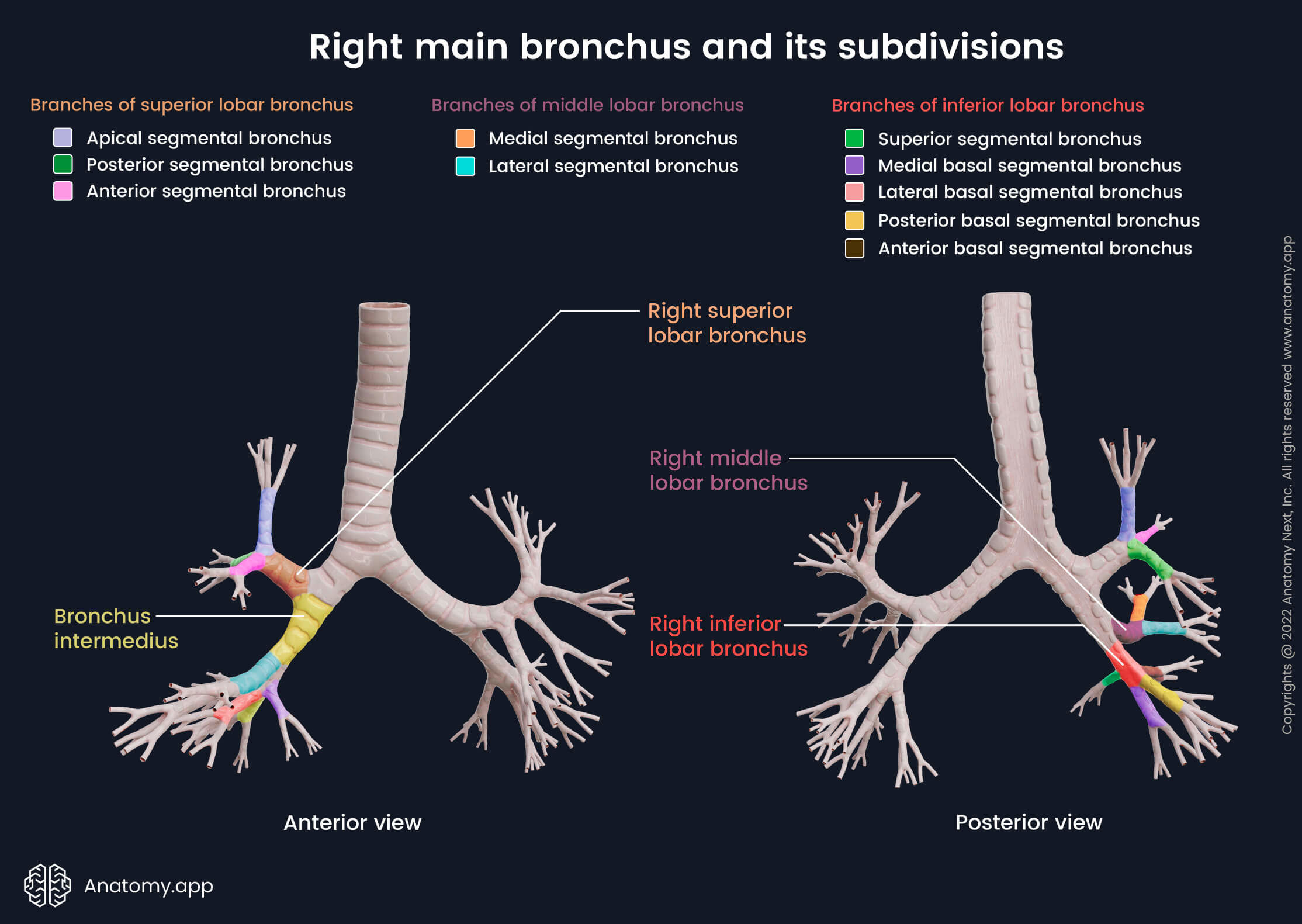
After giving the first branch, the right main bronchus continues further as the bronchus intermedius. It enters the hilum of the lung and there divides itself into two branches - middle and inferior lobar bronchi. Sometimes an additional subsuperior segmental bronchus can be present. Around 2 cm below the branching of the superior lobar bronchus, the bronchus intermedius gives rise to the right middle lobar bronchus. It soon divides into two segmental bronchi:
- Medial segmental bronchus - supplies the middle lobe of the right lung;
- Lateral segmental bronchus - along with the medial segmental bronchus supplies the middle lobe.
After giving the second branch, bronchus intermedius further continues as the right inferior lobar bronchus. The right inferior lobar bronchus gives rise to several segmental bronchi:
- Superior segmental bronchus - supplies the upper part of the inferior lobe;
- Medial basal segmental bronchus - supplies a small region below the hilum of the lung;
- Anterior basal segmental bronchus - supplies the anterior basal segment of the inferior lobe;
- Lateral basal segmental bronchus - supplies the lateral basal segment of the inferior lobe;
- Posterior basal segmental bronchus - supplies the posterior basal segment of the inferior lobe.
Left main bronchus and its subdivisions
The left main bronchus is twice longer, narrower and more horizontal than the right main bronchus. The left main bronchus passes below the aortic arch, and anteriorly relates to the esophagus, thoracic duct and descending thoracic aorta. The left pulmonary artery passes at first above and then in front of the left main bronchus. The left main bronchus gives rise to two lobar bronchi - superior and inferior.
The left superior lobar bronchus divides further into branches headed superiorly and inferiorly, which together supply the whole superior lobe of the left lung. The superior branch ascends and gives off an anterior segmental bronchus and continues further for 1 cm as an apicoposterior segmental bronchus. The apicoposterior segmental bronchus then divides into apical and posterior subdivisions.
The inferior branch of the left superior lobar bronchus is headed downward towards the anterior lower part of the left superior lobe (lingula) and gives off the common lingular bronchus. The common lingular bronchus then soon divides into superior and inferior lingular segmental bronchi. This kind of distribution is different from that of the right lung. The corresponding branches in the right middle lobe head to the medial and lateral bronchopulmonary segments.
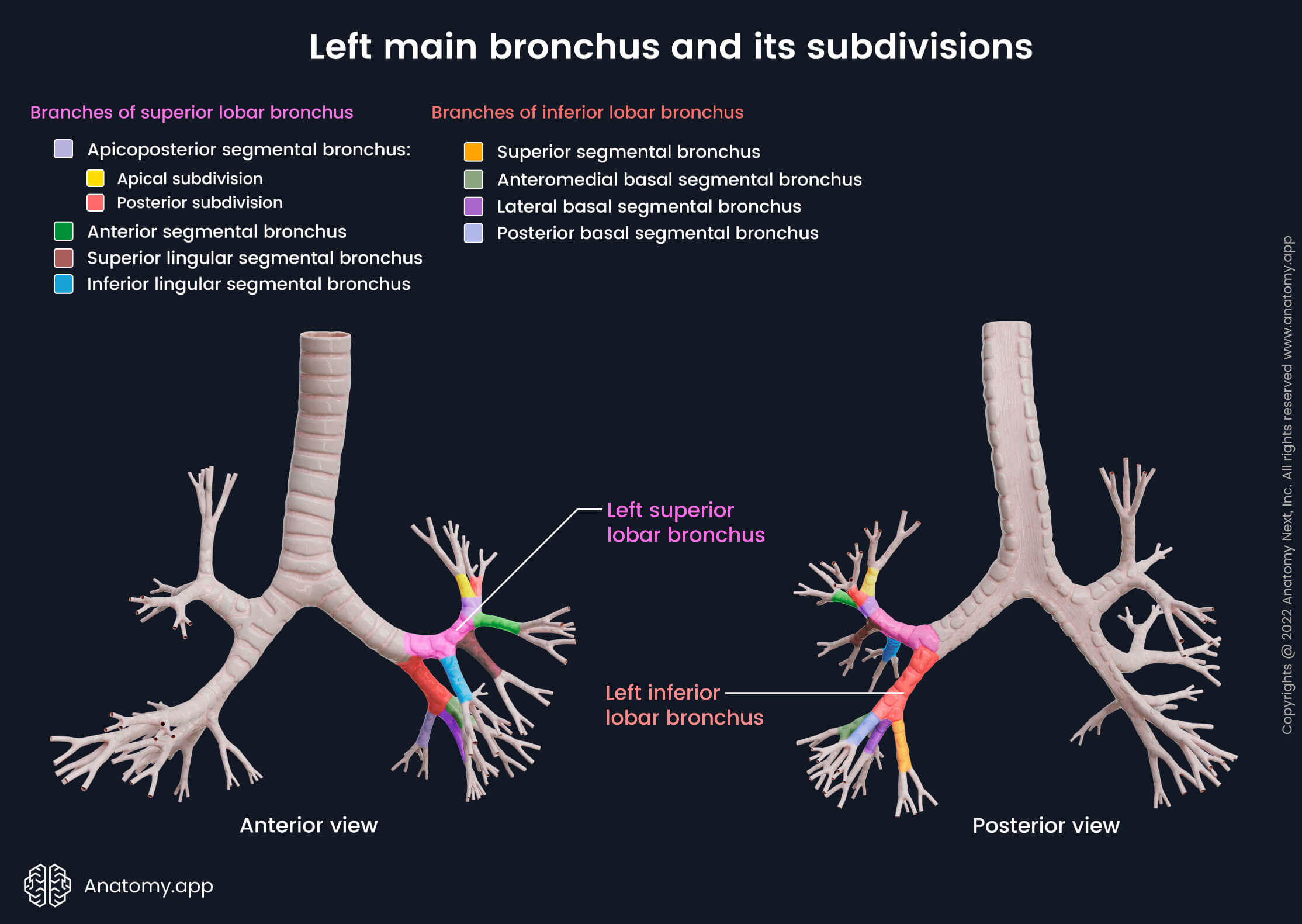
NOTE: Sometimes the left superior lobar bronchus does not give the inferior branch (common lingular bronchus), but instead, the superior and inferior lingular segmental bronchi arise directly from the superior lobar bronchus. You can see this branching pattern in our visual material.
The left inferior lobar bronchus descends posterolaterally and mimics the corresponding branching system of the right lung. The divisions of the left inferior lobar bronchus supply the corresponding bronchopulmonary segments, similar to the right lung. The left inferior lobar bronchus divides into the following bronchi:
- Superior segmental bronchus
- Anteromedial basal segmental bronchus (divides into the anterior and medial basal segmental bronchi)
- Lateral basal segmental bronchus
- Posterior basal segmental bronchus
Histology of bronchi
Like the trachea, the bronchi are lined by a mucosal layer, consisting of respiratory epithelium and supporting lamina propria - a connective tissue layer beneath the epithelium. Under the mucosa lies the submucosal layer. It is made of connective tissue and contains smooth muscle cells, bronchial glands, blood vessels, lymphatics and nerves. The third layer is either the muscular or cartilage layer or both. Large bronchi contain cartilages that are absent starting from the bronchioles. Therefore, bronchi until bronchioles usually have cartilage and muscular layers, while bronchioles present with a muscular layer. And finally, the fourth external layer is adventitia, made of fibrovascular connective tissue.
Mucosal layer
The epithelium of the bronchi is similar to that of the rest of the airways. The bronchi are mainly lined by the respiratory epithelium (pseudostratified columnar ciliated epithelium), containing mucus-secreting goblet cells. Bronchioles are lined by simple columnar to the cuboidal epithelium. The loose connective tissue of the mucosa is composed of many elastic fibers. Six types of cells are found in the non-respiratory conducting part of the airways: ciliated columnar, goblet, Clara, brush, basal and neuroendocrine cells.
- Ciliated columnar cells are the central cells involved in the mucociliary clearance mechanism. Each cell has up to 300 cilia that produce movements. These movements allow the foreign particles and mucus to move out of the airway. The tips of the cilia are immersed into a thick blanket of mucus secreted by the goblet cells and mucous cells from the submucosal glands. There are fewer cilia in the terminal and respiratory bronchioles. The epithelium gradually changes into simple cuboidal epithelium towards the alveoli. Non-ciliary cells become the predominant cells.
- Goblet cells are found in the trachea and up to the smaller bronchi. Goblet cells are absent in bronchioles. The apical zone of the goblet cell is full of secretory vesicles. These cells produce mucinogen - a component of the mucus present in the respiratory tract.
- Clara cells are non-ciliated secretory cells. They are located mainly in the small bronchi. Clara cells produce and secrete surfactant components. Functionally, Clara cells are similar to the type II alveolar cells found in the pulmonary alveoli.
- Brush cells are a relatively rare epithelial cell type. They have long apical microvilli. It is thought that these cells act as sensory receptors since they have contact with afferent nerve ending on their basal surfaces.
- Basal cells are small rounded cells. They rest on the basement membranes. Basal cells serve as stem cells that replace other types of epithelial cells (goblet, brush and ciliated columnar).
- Neuroendocrine cells are located mainly in the basal part of the epithelium, and they are a part of the neuroendocrine system. Neuroendocrine cells are hormone-producing cells that release hormones in response to neural stimuli.
Lymphocytes and mast cells are also found in the airway epithelium. They migrate to the epithelium from the underlying connective tissue.
- T-lymphocytes found within the bronchi mainly come from the mucosa-associated lymphoid tissue (MALT). T-lymphocytes provide immunological functions. They kill and eliminate infected host cells and intracellular microbes, activate other immune cells (macrophages, B cells), regulate immune response and provide cytokine release.
- Mast cells are located in the basal part of the airway epithelium. They contain histamine granules. When triggered by irritants or allergens, they release the granules outside the cell.
Submucosal layer
The submucosal layer is located under the epithelium and lamina propria. It contains seromucous glands situated mainly in the larger bronchi and in the smaller bronchi to a lesser degree. The seromucous glands are made up of serous and mucous cells, and they produce mucus that covers the surface of the ciliated epithelium. Bronchioles do not contain bronchial glands.
The connective tissue of the submucosal layer contains long bands of elastin that form a web. This network of elastic fibers helps to adjust the diameter of the airway to the flow of air. These fibers assist the lungs in returning to the initial state during expiration. The submucosal layer also contains smooth muscle cells.
Muscular and cartilage layers
Bronchi can be classified according to the structure of their walls, and they can be either cartilaginous or muscular bronchi. Larger bronchi contain a significant amount of hyaline cartilages in their walls. As they branch further and divide into smaller bronchi, the amount of cartilage decreases while the number of smooth muscle cells increases.
NOTE: Cartilaginous bronchi contains both layers - cartilage and muscular layers. Therefore, they present with mucosa, submucosa, cartilage layer, muscular layer and adventitia.
The cartilage layer is made of fibrous tissue and individual cartilage plates. The muscular layer is formed by longitudinal and circular bundles of smooth muscle cells. Smooth muscle fibers are controlled by the nervous and hormonal systems. The contraction of smooth muscle cells within bronchi makes the airways narrower during expiration (bronchoconstriction). In contrast, relaxation makes the airways wider during inspiration (bronchodilation).
Neurovascular supply of bronchi
Arterial blood supply
The bronchial arteries supply blood to the bronchi, as well as the trachea, esophagus and fibrous tissue of the lungs. The bronchial arteries most commonly branch off the descending part of the thoracic aorta. They accompany the bronchi up to the level of respiratory bronchioles. Usually, there is one right, and two left (superior and inferior) bronchial arteries.
Venous drainage
Bronchial venous drainage occurs through two systems - superficial and deep. The superficial bronchial veins drain the extrapulmonary bronchi, visceral pleura and hilar lymph nodes. The deep bronchial veins anastomose with the pulmonary veins and together form the intrapulmonary bronchiolar plexus. Usually, two bronchial veins on each side are draining the venous blood from larger bronchi and hilar structures.
The superficial bronchial veins drain into the azygos vein on the right side, left superior intercostal vein or the accessory hemiazygos vein on the left side. The deep bronchial veins drain into the pulmonary veins or directly into the left atrium of the heart. Nevertheless, the majority of the blood supplied from the bronchial arteries returns through the pulmonary veins and, to a lesser extent - the bronchial veins.
Lymphatic drainage
The lymphatic drainage originates from the bronchioles and their surrounding plexuses. Lymph node groups are located along with the divisions of the bronchial tree. The peripheral lymph is drained into the hilar nodes and further into the tracheobronchial lymph node groups along the sides of the trachea. The vessels from these nodes merge together with the vessels from the brachiocephalic and parasternal nodes, forming right and left bronchomediastinal trunks.
Innervation
Innervation of the bronchi happens via anterior and posterior pulmonary plexuses. They are located around the hila of the lungs in front of and behind the tracheal bifurcation and main bronchi, anastomosing with each other. The plexuses are formed mainly by branches of the vagus nerve (CN X) and sympathetic trunks. The efferent fibers from the vagus nerve are parasympathetic and participate in the narrowing (constriction) of the airways. The efferent fibers of the sympathetic trunks participate in the widening (dilation) of the airways.
Disorders of bronchi
Bronchial pathology can manifest in various ways. The most common diseases of the bronchi include bronchitis (acute and chronic) and bronchial asthma. Acute bronchitis is a transient inflammation affecting the bronchi. It is accompanied by a cough that is dry or productive (with mucus). Acute bronchitis is an infectious disease, most often caused by viruses.
It is usually self-limiting, although recovery is very slow (10- 20 days). It does not require any medical treatment, and, typically, antibiotics are not necessary. When the cough is present at least three months and happens multiple times over two years, it is referred to as chronic bronchitis. Chronic bronchitis is most commonly seen in smokers. (Read more about the cough reflex and the effects of smoking on the airways in our article on the trachea!)
Bronchial asthma (or simply asthma) is a chronic inflammatory condition that affects the airways of the lungs and causes occasional breathing difficulties. It involves airway inflammation, obstruction and bronchial hyperresponsiveness. The typical signs of asthma are coughing, shortness of breath, tightness in the chest and wheezing. Asthma is treated mainly by inhalers. The inhalers contain such medications as bronchodilators that dilate (widen) the bronchi and corticosteroids used to decrease bronchial inflammation.
Asthma is among the most common chronic diseases worldwide, especially among children. It is a significant public health problem. Due to restricted activities, asthma holds a negative impact on the quality of life of the individual and society. It also largely burdens the healthcare system because of the many emergency department visits and hospitalizations of asthmatic patients.
References:
- Broaddus, V. C., Ernst, J., King, T., & Lazarus, S. (2021). Murray & Nadel’s Textbook of Respiratory Medicine, 2-Volume Set (7th ed.). Elsevier.
- Drake, R., Vogl, W., & Mitchell, A. (2019). Gray’s Anatomy for Students: With Student Consult Online Access (4th ed.). Elsevier.
- Fayyaz, D. J. O. (2021, July 12). Bronchitis: Practice Essentials, Background, Pathophysiology. Medscape. https://emedicine.medscape.com/article/297108-overview
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Haschek, W. M., Rousseaux, C. G., Wallig, M. A., & Bolon, B. (2021). Haschek and Rousseaux’s Handbook of Toxicologic Pathology. Elsevier Gezondheidszorg.
- Morris, M. J. (2021, May 3). Asthma: Practice Essentials, Background, Anatomy. Medscape. https://emedicine.medscape.com/article/296301-overview
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app