- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
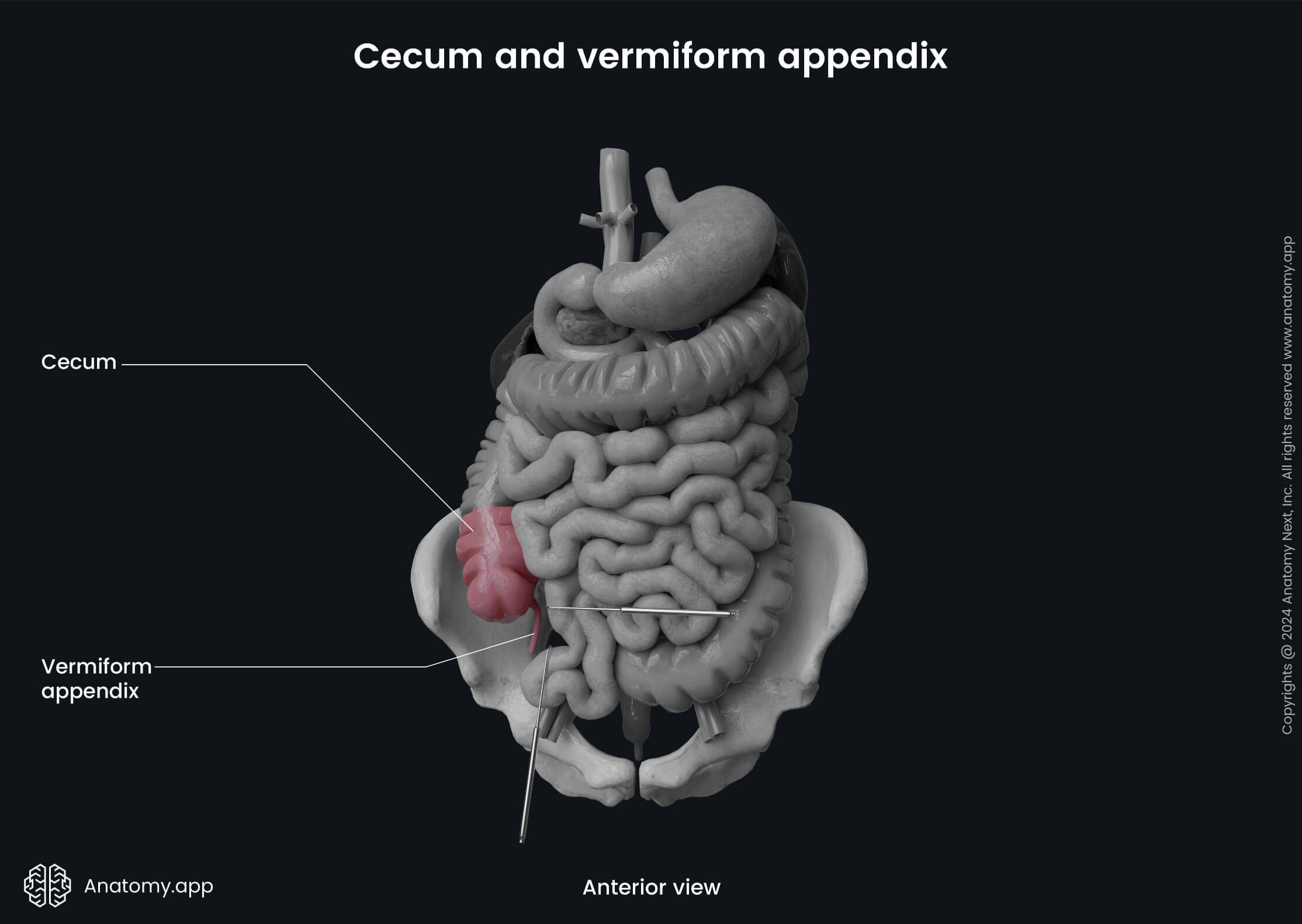
Cecum and vermiform appendix
The cecum (Latin: caecum) is the first and most proximal part of the large intestine connecting the ileum with the ascending colon. It is a sac-like or pouch-shaped organ located in the abdominal cavity. The cecum starts the absorption of remaining water and salts. From the posteromedial surface of the cecum extends the cylindric-shaped vermiform appendix (Latin: appendix vermiformis), mostly providing immunologic function.
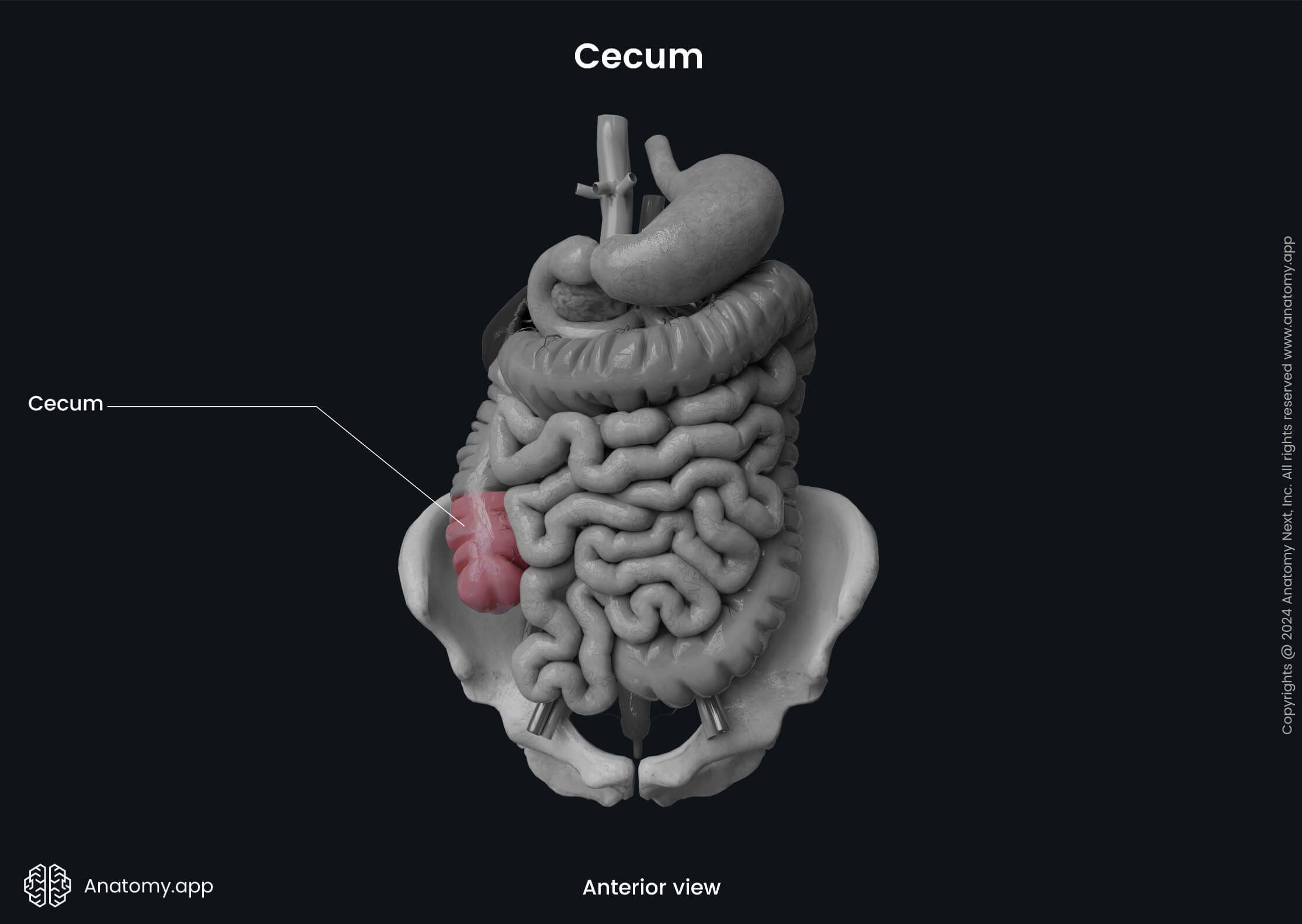
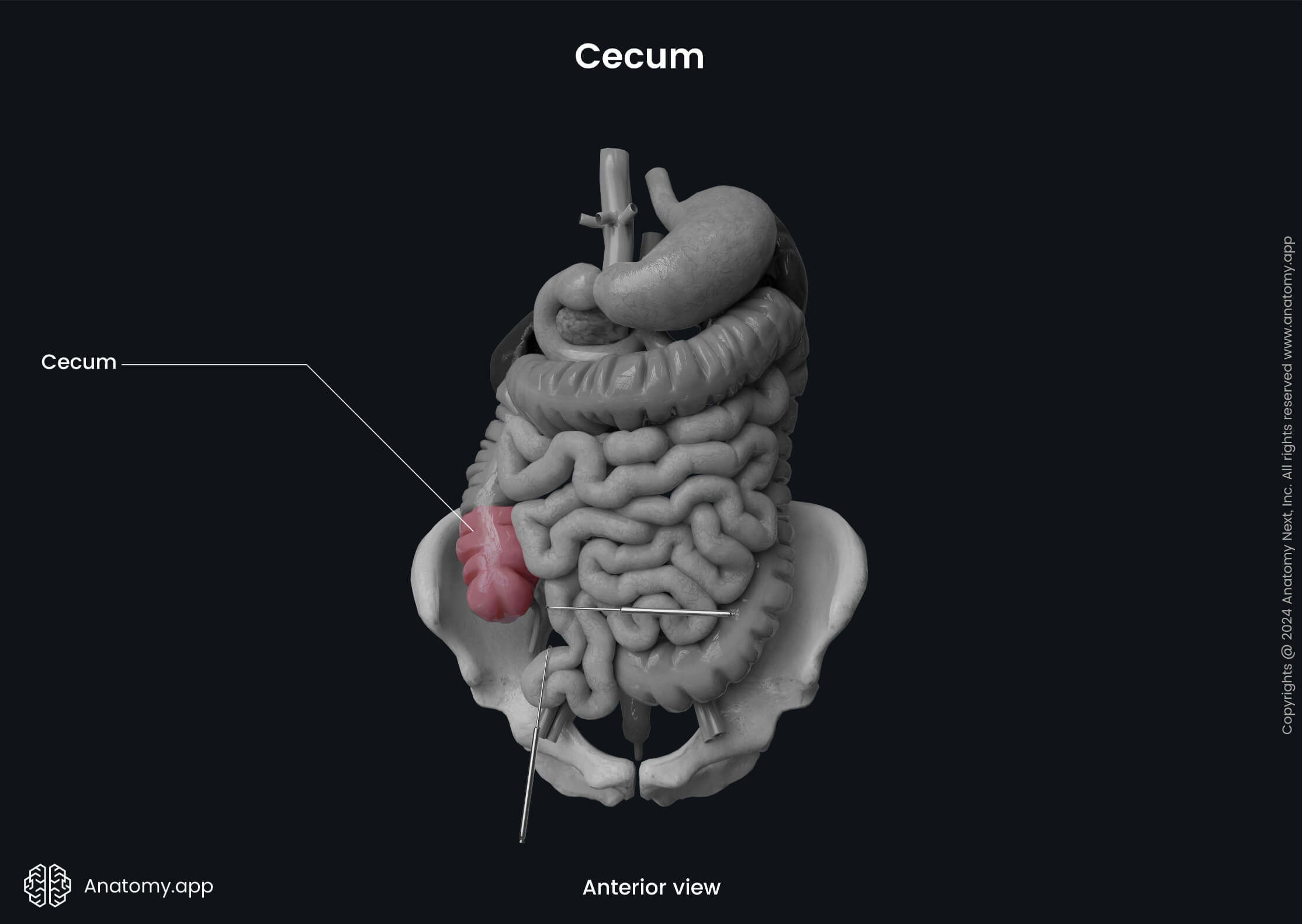
Cecum anatomy
The cecum is located in the right iliac fossa, which is found in the right inguinal region. The organ is approximately 2 - 2.8 inches (5 - 7 cm) long with a diameter of 2.8 to 3 inches (7 - 7.5 cm), so it is usually wider than its length. The ileum, which is the terminal part of the small intestine, is connected with the cecum on its medial surface at the ileocecal junction. The junction place has an opening - ileocecal orifice. The orifice contains the ileocecal valve.
The ileocecal valve (also known as the Bauhin’s valve) demarcates the transition zone between the small and large intestines. It is more a functional valve, preventing the intestinal content backflow from the large intestine into the small intestine. But it can not control the movement of gut content from the ileum to the cecum. The valve is made up of the circular muscle fibers of the cecum and ileum.
The visceral layer of the peritoneum covers the cecum from all sides. Therefore, the cecum is an intraperitoneal organ. The cecum does not have a mesentery, and that is why it is very mobile.
Anatomical relations
Posterior to the cecum are situated the iliacus and psoas major muscles, lateral femoral cutaneous nerve, femoral nerve and genitofemoral nerve. The anterior surface of the cecum is connected with the wall of the abdomen. Sometimes, it can also connect with the greater omentum and loops of the small intestine.
Superiorly, the cecum continues as ascending colon, but inferiorly it is related to the part of the inguinal ligament. Medial to the cecum is the ileocecal valve and the terminal part of the ileum.
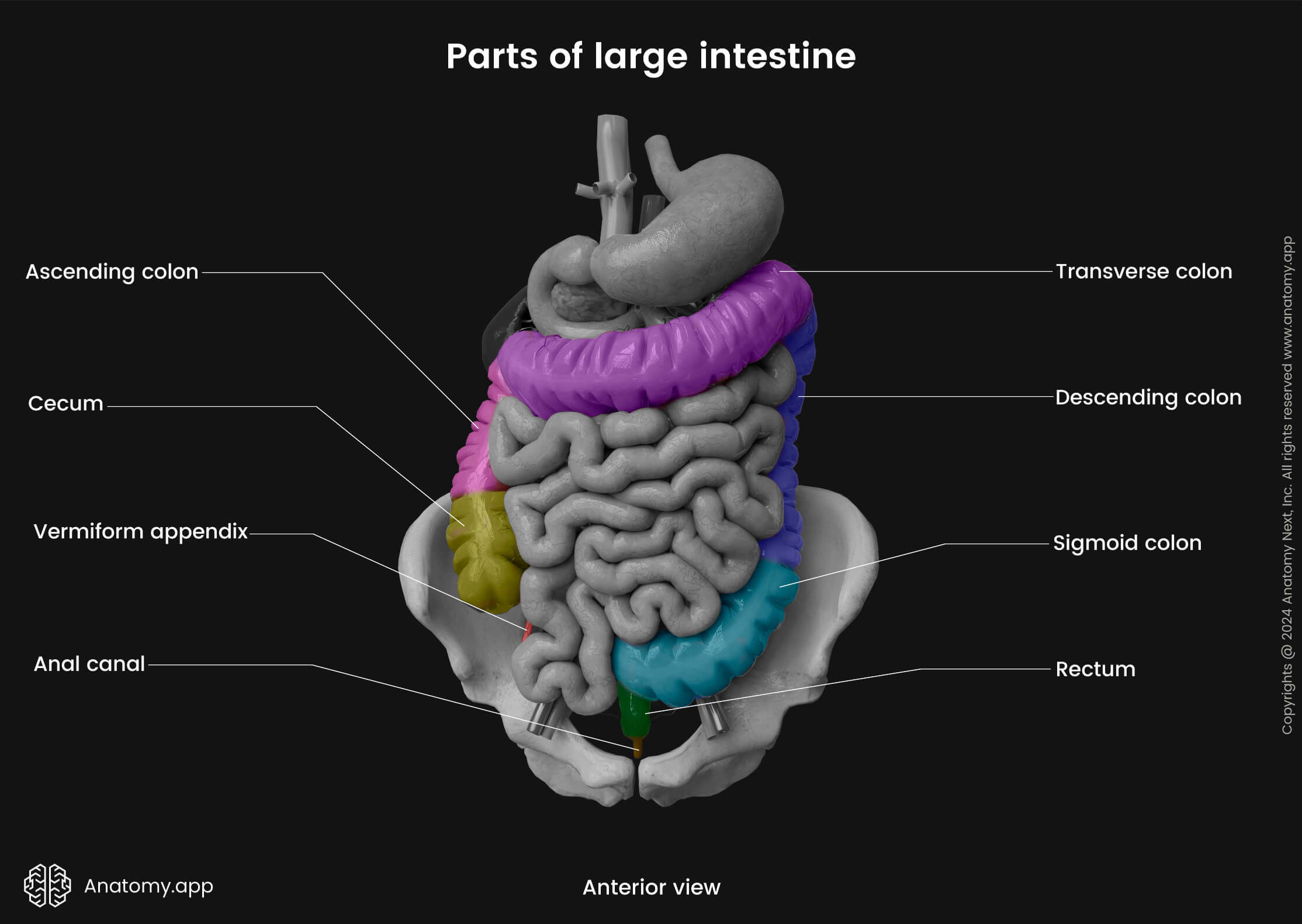
Characteristics of large intestine
Almost all parts of the large intestine have typical characteristics. Therefore also, the cecum has haustra, teniae and epiploic appendages.
Haustra
The wall of the cecum is arranged into pocket-like sacs or small segmented pouches caused by sacculation of the large intestine. The sacs are called haustra, and they give the intestine its segmented appearance. At the sites where two haustra meet, crescent-shaped folds called semilunar folds can be found. They are made of the mucosal and submucosal layers of the intestinal wall. However, the haustra are more pronounced in other parts of the large intestine, especially towards the sigmoid colon, while often absent in the cecum.
Teniae
The outer muscular layer of the large intestine forms three narrow longitudinal bands known as taeniae coli. Overall, the large intestine has three types of taeniae:
- Mesocolic taeniae - located posteromedially; correspond to the attachment of the mesentery; the transverse mesocolon and sigmoid mesocolon attach to them;
- Omental taeniae - situated posterolaterally and serve for the attachment of the greater omentum;
- Free taeniae - positioned on the anterior side of the intestine and are not attached to any structure.
All taeniae contain smooth muscle cells. Contractions of muscle fibers cause shortening of the large intestine wall, leading to the formation of the previously described segmented sacs (haustra) between the taeniae. The taeniae of the cecum converge at the base of the vermiform appendix, making it easier for a surgeon to localize the appendix during surgery.
Epiploic appendages
The outer surface of the large intestine along the free and omental taeniae has epiploic appendices that are small fat-filled projections of the peritoneum. They are found along the entire length of the large intestine. However, they are more pronounced in the distal parts of the colon and are rarely present in the cecum.
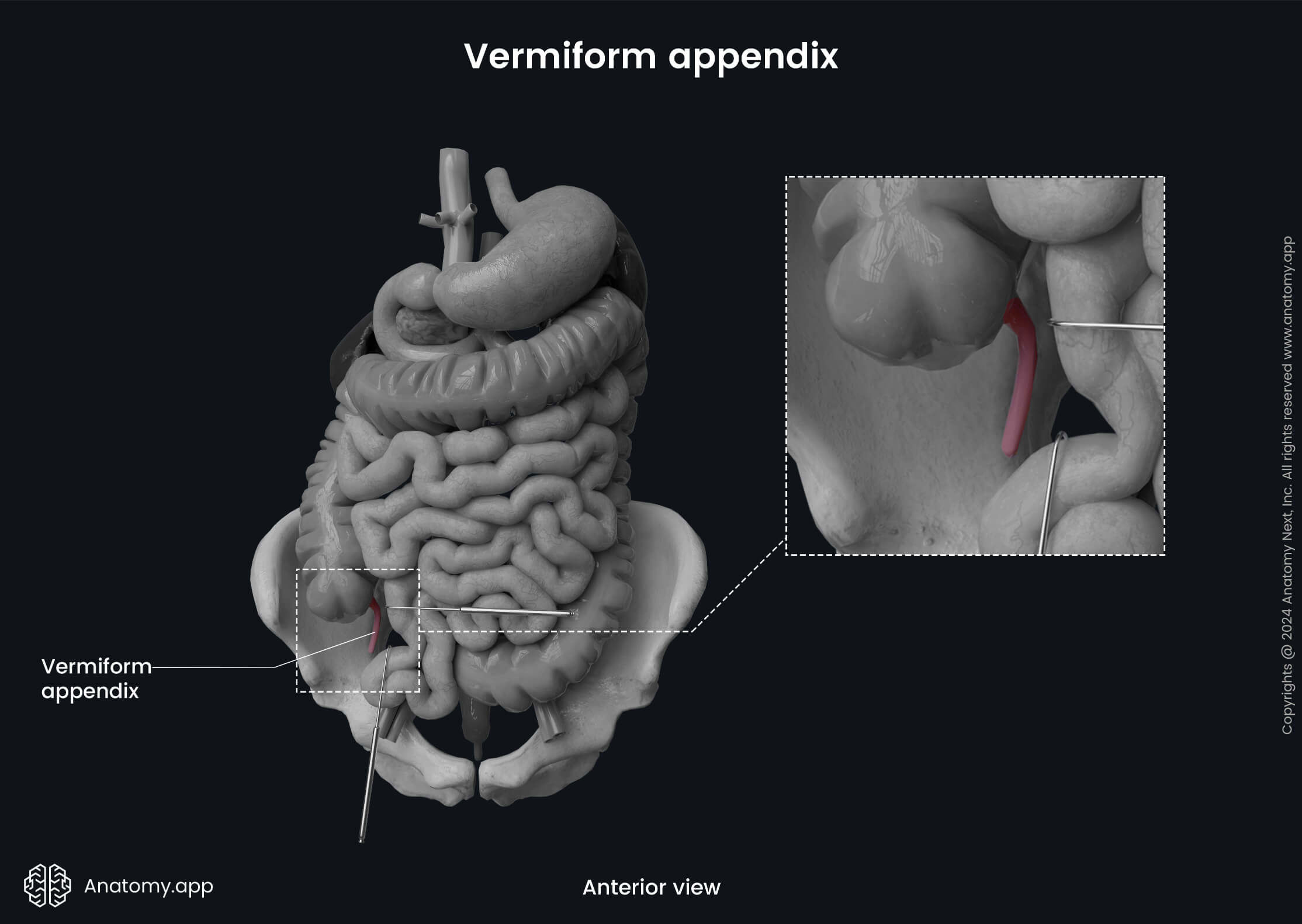
Vermiform appendix anatomy
The vermiform appendix is a narrow tube-like structure with a blind end. The Latin word vermiform actually means "worm-like in form" because its shape resembles that of a worm. It is usually 2.5 - 4 inches (6 - 10 cm) long. However, the structure is quite variable in its length - it can range from 0.8 up to 8 inches (2 - 20 cm). The diameter usually is around 0.2 to 0.4 inches (0.5 - 1 cm). The appendix contains massive amounts of lymphoreticular tissue; therefore, it primarily provides immunological function.
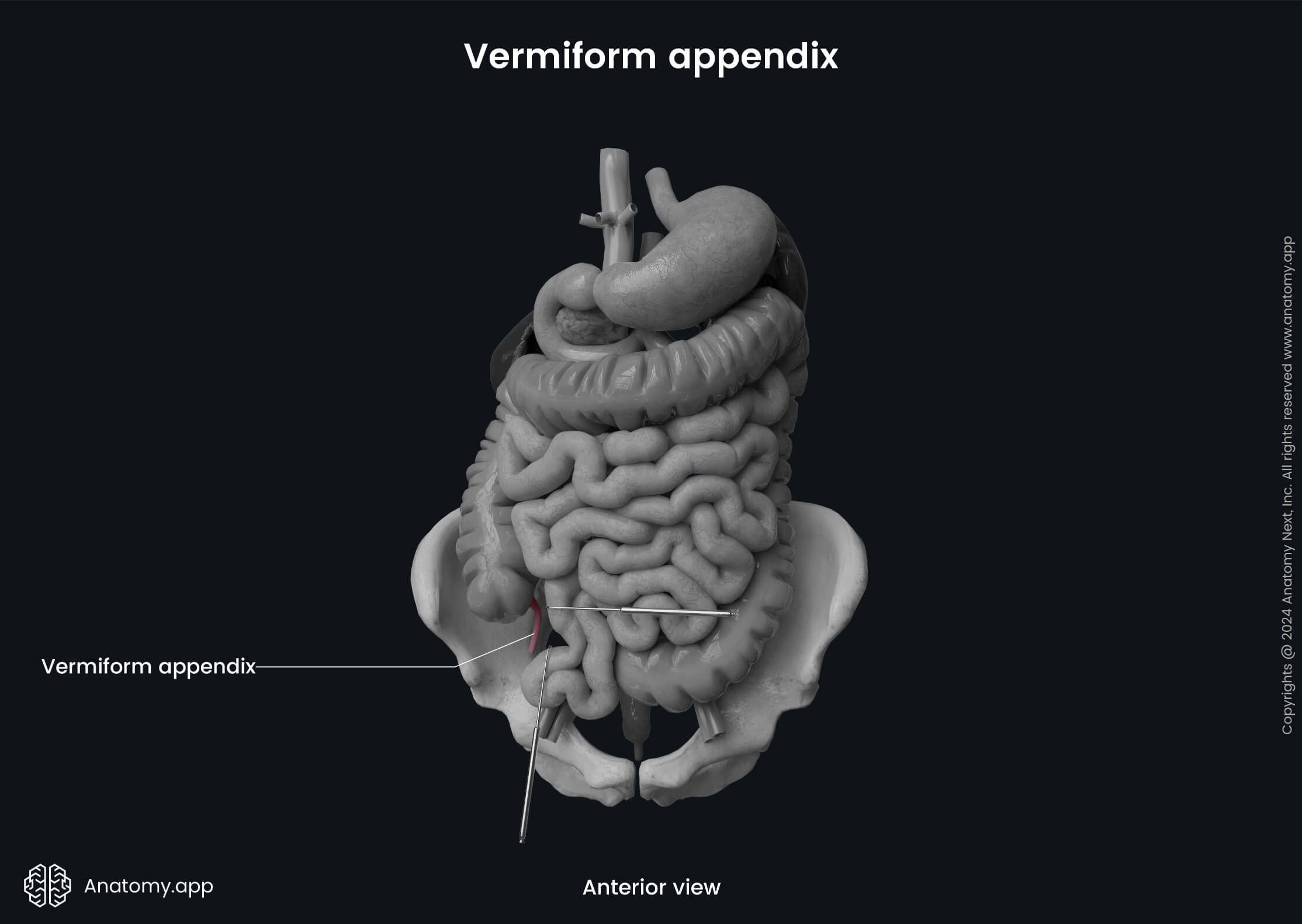
The appendix extends from the posteromedial wall of the cecum, usually 0.4 - 1.2 inches (1 - 3 cm) below the ileocecal junction. Along with the cecum, it is also situated in the right iliac fossa, but its distal tip can extend as far as the liver and its location can be quite variable. The vermiform appendix has an opening called the vermiform appendix orifice at the site where it connects with the cecum. Usually, the anterior surface of the appendix is covered by the small intestine. But sometimes, it is connected with the abdominal wall.
The appendix is an intraperitoneal organ, as it is covered by the visceral layer of the peritoneum from all sides, and it has a triangular-shaped mesentery called the mesoappendix. The mesoappendix attaches the vermiform appendix to the terminal ileum and is derived from it. Sometimes it is also attached to the posterior abdominal wall in the area of the ileocecal junction. The vermiform appendix does not have characteristic features of the large intestine, such as the previously described teniae, haustra, and epiploic appendages.
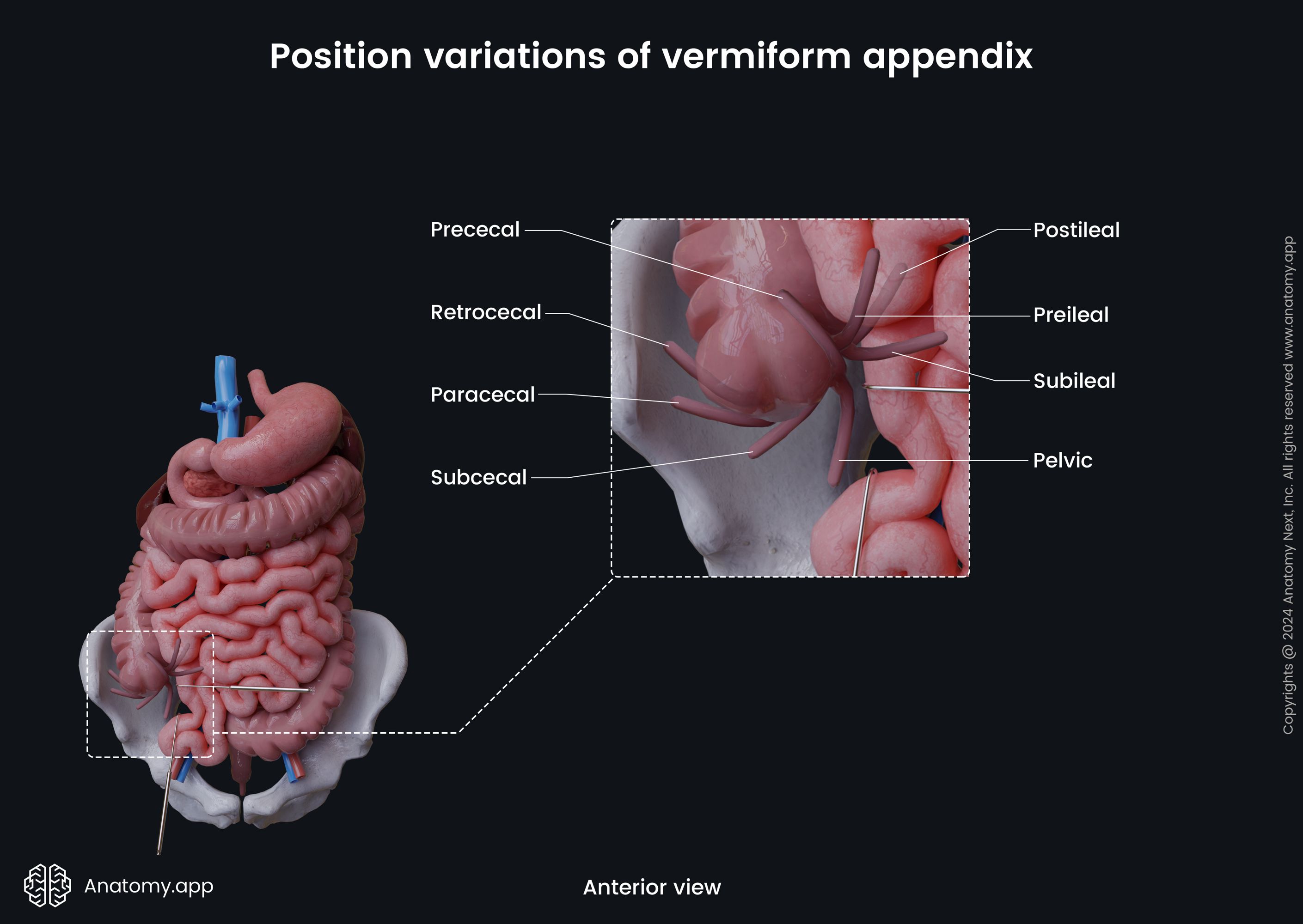
Position variations of vermiform appendix
The vermiform appendix can have different position variations among individuals. Usually, the vermiform appendix has a retrocecal position, meaning it is located behind the cecum. Sometimes it can descend towards the lesser pelvis and pass even below the linea terminalis. In that case, its location is termed pelvic or caudal. It can rarely be subcecal (below the cecum) or preileal (in front of the terminal ileum). The mentioned variations and some other positions are described below.
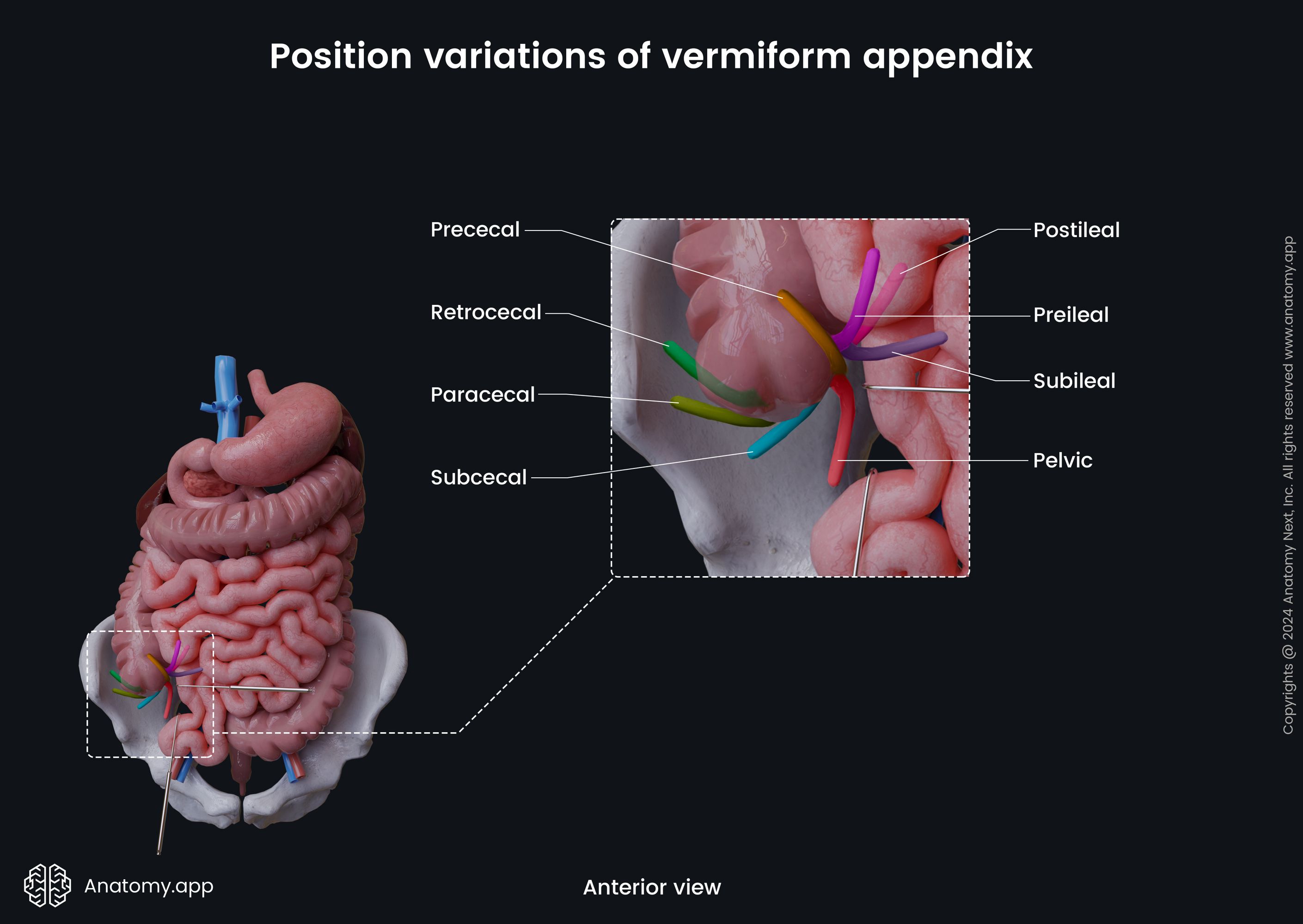
- Retrocecal position or posterior location - as mentioned, it is the most common one. The appendix passes posterior to the cecum. In this case, it can turn upward and reach the right kidney or the liver. If this location is present, the appendix can also fuse with the wall of the cecum.
- Pelvic position is also seen relatively often. The vermiform appendix extends downward in the direction of the lesser pelvis. It crosses the terminal line, and inferiorly has a connection with the rectum, bladder, as well as the right ovary and right uterine tube in females.
- Preilial position - in this case, the appendix is located anterior to the terminal part of the ileum.
- Postileal position - the appendix is situated posterior to the terminal ileum.
- Subileal location - present when the appendix goes parallel to the terminal ileum.
- Subcecal position - when the appendix goes below the cecum.
- Paracecal postition - the appendix passes along the lateral surface of the cecum.
- Prececal position - the rarest location of the appendix, when it is located on the anterior surface of the caecum.
Clinical note: The vermiform appendix can be palpated through the abdominal wall in the lower right quadrant of the abdomen in a site called McBurney’s point. If an imaginary line is drawn from the anterior superior iliac spine to the umbilicus, McBurney’s point is located one-third of the distance laterally. Tenderness or pain localized at this point or near it can signify appendicitis - inflammation of the appendix.
Cecum and appendix histology
The walls of the cecum and vermiform appendix consists of four histological layers:
- Mucosa
- Submucosa
- Muscular layer
- Serosa
Mucosa
The mucosa of the cecum and appendix is covered by simple columnar epithelium. Underneath the epithelium is the lamina propria containing loose connective tissue and the so-called sub-epithelial collagen table with collagen fibers. The mucosa also has prominent muscular lamina (beneath the lamina propria) with smooth muscle fibers forming the outer longitudinal and inner circular layers.
The mucosal membrane is very thick, and together with the submucosa, it creates semilunar mucosal folds at the sites where two haustra meet. The cecum contains slight folds compared to other parts. The vermiform appendix does not have the mentioned folds, and its mucosa is smooth.
In contrast to the small intestine, the cecum does not contain villi and circular folds. The large intestine contains more crypts than the small intestine does. They are deeper and placed more densely. The cecum contains the lowest crypts in height compared to other parts of the large intestine.
The epithelial cells of the large intestine are called colonocytes. Besides colonocytes, the epithelium also contains a significant amount of the goblet cells producing mucus. The crypt base contains simple tubular glands, also known as the Lieberkuhn crypts. The crypts contain various cell types, such as the following:
- Epithelium stem cells - provide the regeneration of epithelium;
- Colonocytes - secrete and absorb multiple substances
- Goblet cells - produce mucus;
- Paneth cells - produce antibacterial substances;
- Endocrine cells - provide secretion of hormones.
Compared to the small intestine, the large intestine rarely contains the Paneth cells. But the large intestine contains significant amounts of goblet cells and stem cells as they often differentiate into goblet cells. The ratio between colonocytes and goblet cells in the cecum is around 4:1.
The mucosa contains solitary lymphoreticular intestinal tissue. Solitary tissue often forms larger follicles in the mucosa with a continuation in the submucosa. The mucosa of the vermiform appendix contains a significant amount of lymphoid tissue grouped in lymphoreticular tissue aggregates. Because of the massive lymphoid tissue amount, the appendix was formerly called the abdominal tonsil. These aggregates can be found not only in mucosa but also in submucosa .
Submucosa
The submucosa of the cecum and appendix is very well developed and contains irregular connective and adipose tissue. It has a strong connection with the mucosa and muscular layers. The tissue includes lymphatic and blood vessels, ganglion cells, and nerve fibers forming two submucosal nerve plexuses - the Meissner’s and Henle’s plexuses.
Muscular layer
The muscular layer consists of two sublayers - the inner circular layer, and the outer longitudinal layer. As mentioned before, the longitudinal layer forms three flat bands called the teniae coli. Between the teniae, the longitudinal layer is half of the thickness of the circular layer. The vermiform appendix does not contain teniae.
Between the circular and longitudinal muscular layers are nerve fibers forming the Auerbach’s nerve plexus. This nerve plexus contains thick bundles of nerve fibers participating in reflexes. When the chyme passes into the cecum from the ileum, the colon gets signals to activate its motor function.
The vermiform appendix has an irregular composition of the muscular layer. Its wall presents the muscular layer only at the sites where there are no lymphoreticular aggregates. For this reason it looks like the submucosa merges with the muscular layer in the wall of the appendix.
Serosa
As mentioned before, the visceral layer of the peritoneum covers the cecum and the vermiform appendix from all sides. It creates the outer layer of the intestinal wall known as the serosa. The serosa is lined by the mesothelium, which is a single layer of squamous epithelium, and supporting loose connective tissue beneath it.
Neurovascular supply of cecum and appendix
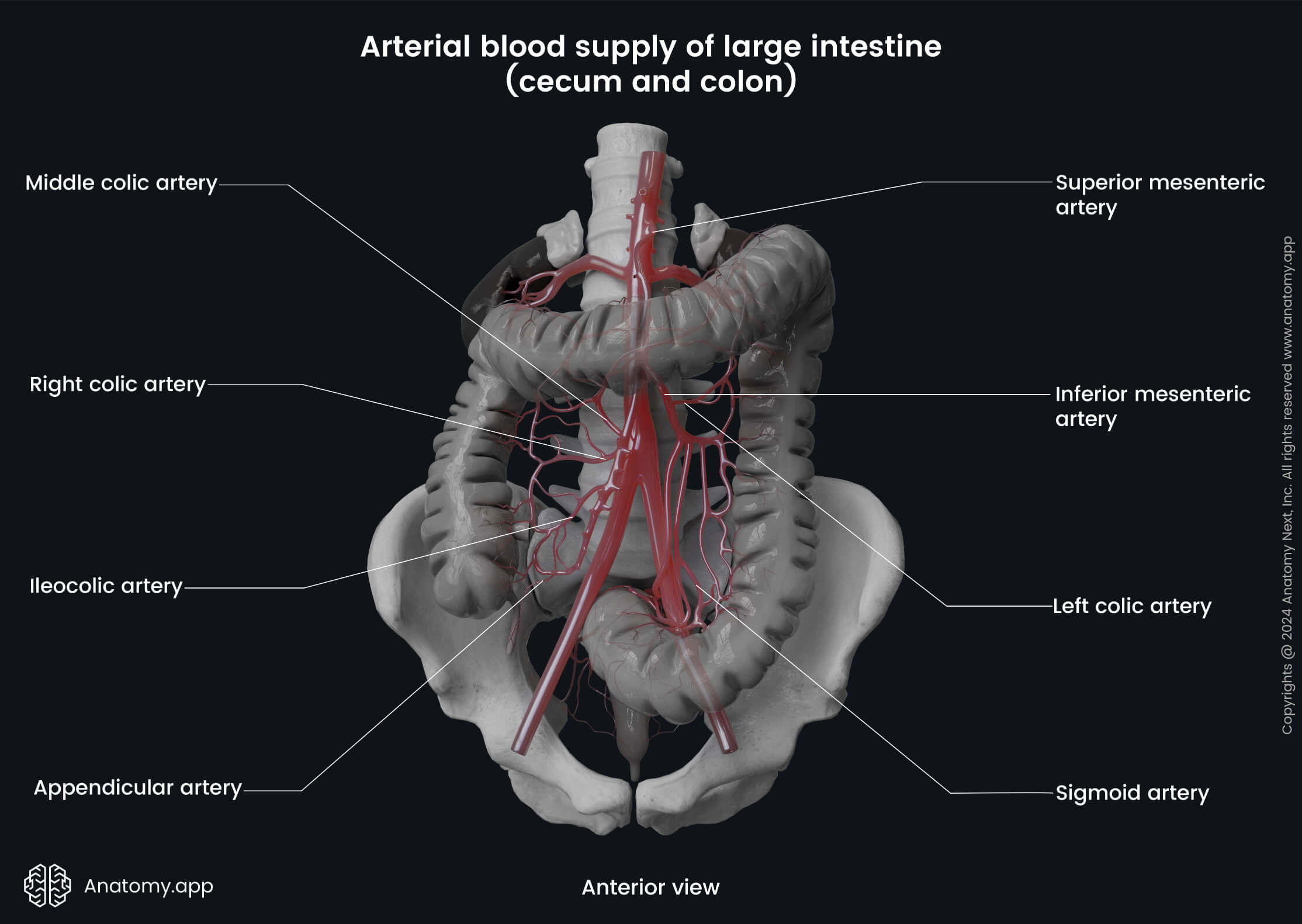
Arterial blood supply
The arterial blood supply of the cecum is provided by the anterior and posterior cecal branches of the ileocolic artery. The ileocolic artery is a branch of the superior mesenteric artery. The vermiform appendix is supplied by the appendicular branch arising from the ileocolic artery.
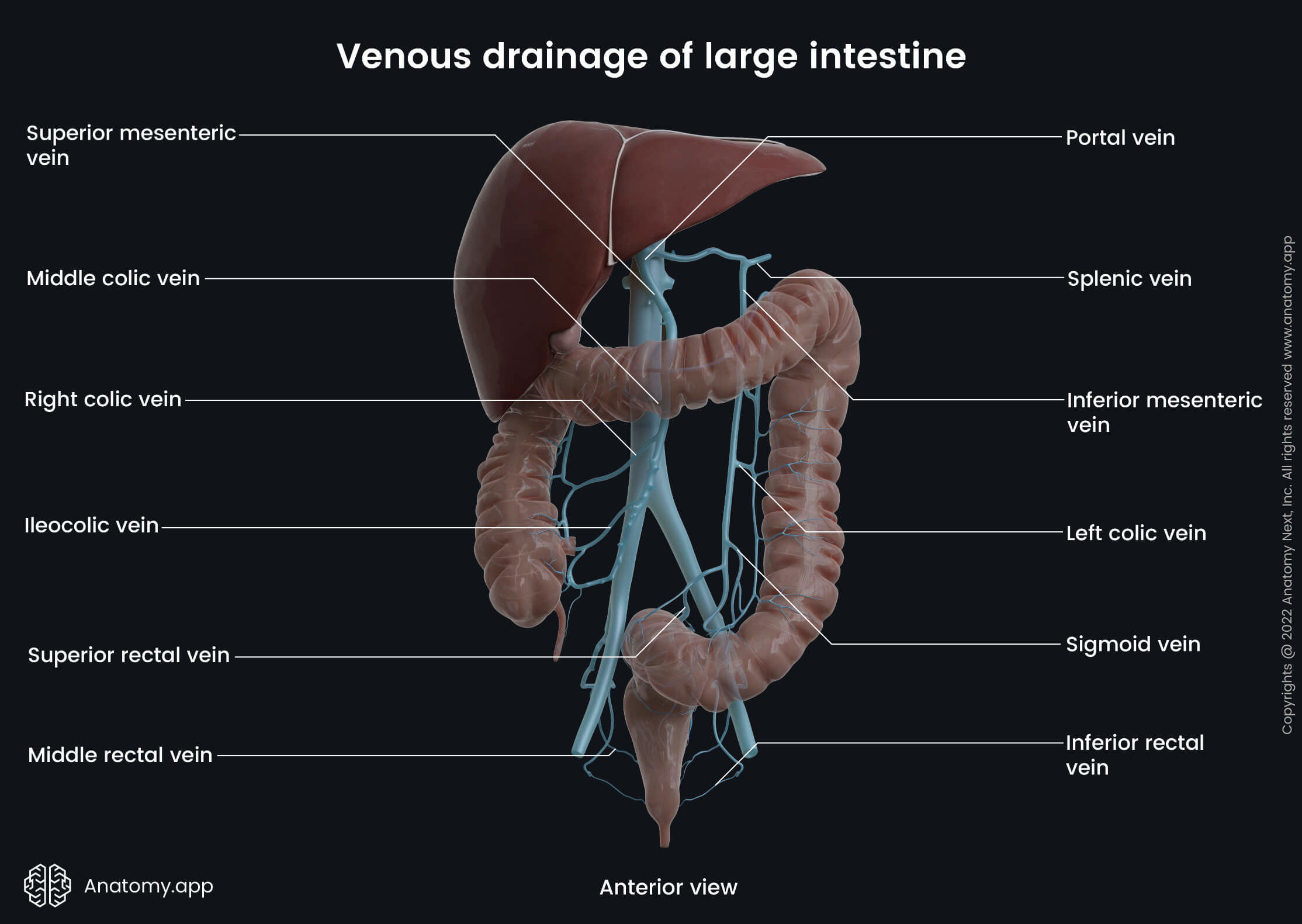
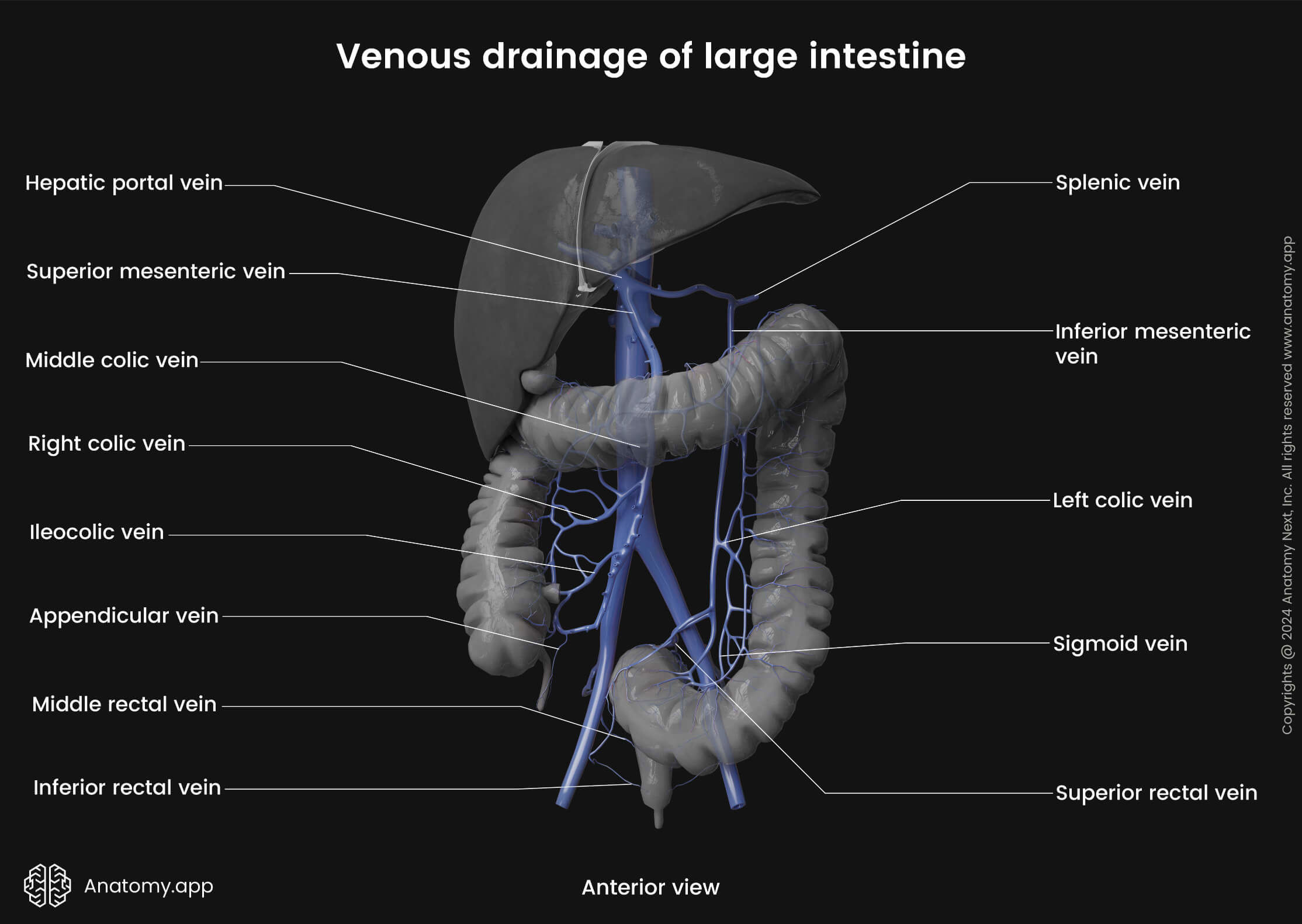
Venous drainage
The venous drainage of the cecum and appendix is provided by the cecal veins draining into the ileocolic vein and next to the superior mesenteric vein. From the superior mesenteric vein blood is carried next to the portal vein.
Lymphatic drainage
Lymphatic drainage from the cecum happens mainly via the superior mesenteric lymph nodes.
Innervation
Parasympathetic innervation of the cecum and appendix is provided by the vagus nerve (CN X). But the sympathetic innervation comes from the superior mesenteric plexus.
Cecum and appendix functions
Like the rest of the large intestine, the cecum provides the absorption of remaining water and salts, which has not been absorbed in the small intestine. The cecum also works as a reservoir for the chyme that is received from the ileum.
The cecum participates in cellulose digestion. In the cecum, the ingredients of food rich in plants are decomposed by bacteria. The bacteria found in the cecum provide fermentation of carbohydrates. As the cecum contains mucus-producing cells, it participates in the lubrication of the intestinal lining that helps to move the gut content further.
The vermiform appendix contains a massive amount of lymphoreticular tissue. Therefore, it primarily plays role in providing mucosal immunity. The appendix is also involved in maintenance of the gut microbiome.
References:
- Drake, R., Vogl, W., & Mitchell, A. (2019). Gray’s Anatomy for Students: With Student Consult Online Access (4th ed.). Elsevier.
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Moore, K.L., Dalley, A.F., Agur, A.M. (2018). Clinically Oriented Anatomy, 8th Edition, Lippincott Williams & Wilkins.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app