- Anatomical terminology
- Skeletal system
- Joints
- Muscles
-
Head muscles
- Extraocular muscles
-
Facial muscles
- Occipitofrontalis
- Corrugator supercilii
- Depressor supercilii
- Orbicularis oculi
- Malaris
- Buccinator
- Orbicularis oris
- Mentalis
- Depressor anguli oris
- Depressor labii inferioris
- Levator anguli oris
- Levator labii superioris
- Risorius
- Zygomaticus major
- Zygomaticus minor
- Levator labii superioris alaeque nasi
- Nasalis
- Procerus
- Depressor septi nasi
- Compressor narium minor
- Dilator naris anterior
- Muscles of mastication
- Neck muscles
- Muscles of upper limb
- Thoracic muscles
- Muscles of back
- Muscles of lower limb
-
Head muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
Malaris
The malaris muscle is a less commonly discussed and researched facial muscle. It is not very well known as not everyone has it. It is more commonly found in East Asian populations such as Koreans. Also, Caucasians show significant numbers of the malaris muscle. Although only a little research has been done on the malaris muscle, it appears to be a significant muscle in the anatomy of the midface and could play a role in midface aging prevention, as well as it could be an anti-aging link of the midface.
The malaris muscle was first observed and described in the literature in 1871 by the German anatomist Henle. He reported a muscular structure consisting of two bands that extend between the superficial temporal fascia and the fat of the cheek. Another description was made by Ligtholler in 1927 - he described the malaris muscle in Australian Aboriginals. According to him, Australian Aboriginals demonstrated muscular structures that originated in the temporal fossa, passed over the zygomaticus major and zygomaticus minor muscles and ended in the labial commissure.
The malaris muscle appears as fine, superficial muscular bands that lie adjacent to the main bulk of the orbicularis oculi. It is found between the orbital area and the upper cheek, playing a crucial role in the appearance and facial expression of the midface region.
Although little is known about the variations of the malaris muscle, current studies show that it is variable among individuals. Sometimes, only a few muscular fibers are found. In contrast, fetuses most commonly have large and bulky malaris muscles. Additionally, anatomical studies have shown that this muscle tends to become atrophic and disappear with age.
The impact of the malaris on the aesthetics of the lower eyelid and cheek makes it an essential muscle for both clinical and surgical considerations. Moreover, understanding the anatomy of the malaris muscle is essential for effective facial procedures and treatments. Aging changes in the malaris muscle can cause the formation of wrinkles, malar bags, or festoons.
Structure and attachment sites
As mentioned previously, the malaris muscle has various morphological appearances. Despite varying anatomical descriptions, it is generally described as a thin muscle sheet that arises in close proximity to the orbicularis oculi (Oo) and extends downward. Current studies show that the malaris muscle may consist of three muscle bands named the medial, lateral, and suspending bands. While the lateral and medial bands are always present, the suspending bands may be missing.
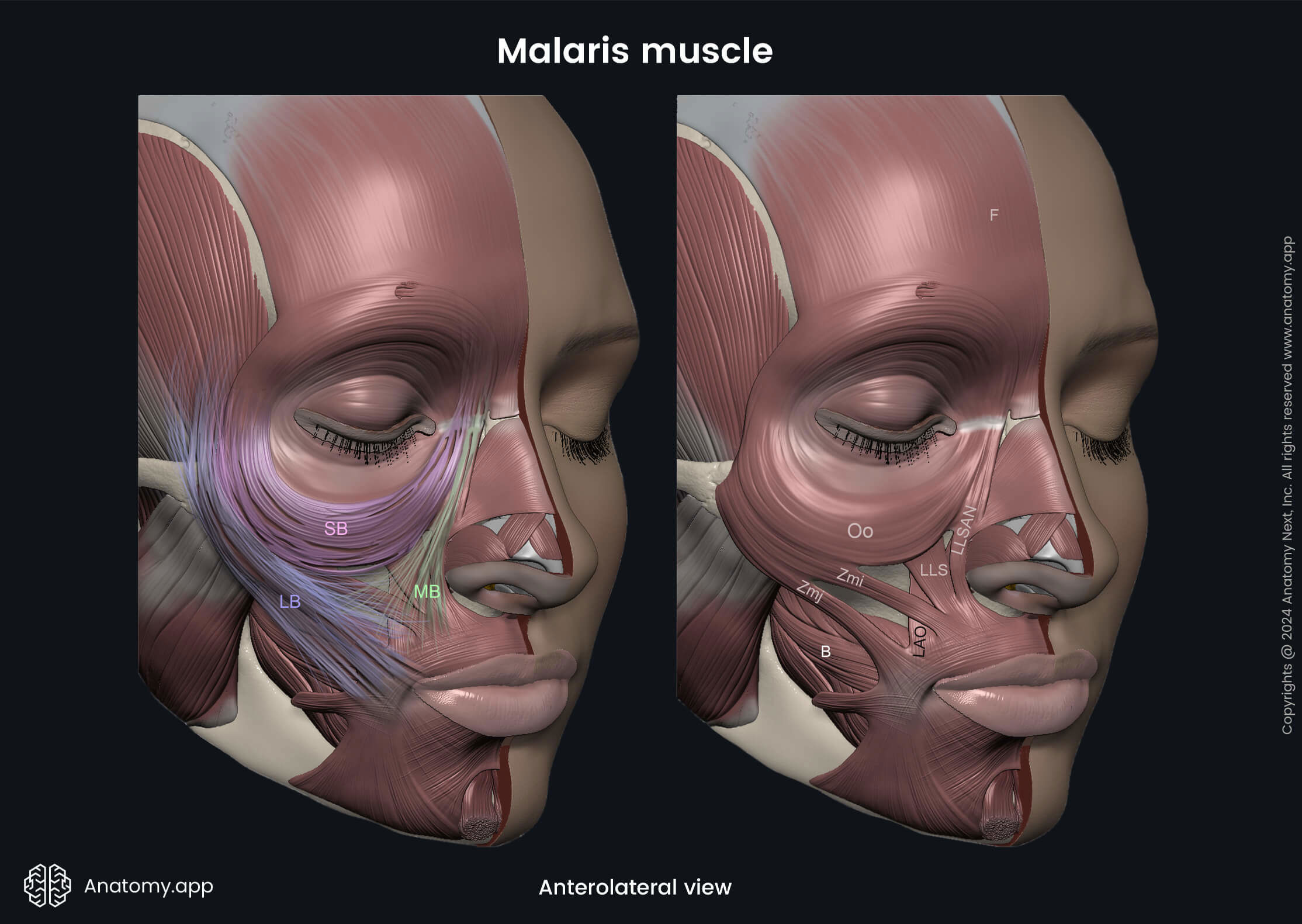
The medial band (MB) is a muscle strand that is found medially to the orbital part of the orbicularis oculi muscle (Oo). It arises from the frontal process of the maxilla, the medial palpebral ligament, and the frontal belly (F) of the occipitofrontalis muscle. From the origin site, the fibers of this band run downward and laterally. This band ends by attaching to the superficial fascia of the cheek, as well as the levator labii superioris alaeque nasi (LLSAN) and levator labii superioris (LLS) muscles.
The lateral band (LB) is a muscle strip that is found adjacent and lateral to the orbital part of the orbicularis oculi muscle (Oo). It arises from the superficial temporal fascia. From the fascia, the fibers of the lateral bundle further pass downward and medially and end by attaching to the superficial fascia of the cheek, zygomaticus minor (Zmi) and zygomaticus major (Zmj) muscles, as well as some fibers may also extend toward the angle of the mouth and the platysma.
The suspending band (SB) was first described recently by Kampan et al. According to Kampan, it is a U-shaped muscle band that is found inferior to the orbital part of the orbicularis oculi muscle (Oo). Interestingly, the attachment sites of the suspending band on the medial and lateral sides match the proximal attachments of the medial and lateral bundles of the malaris muscle. Medially, the suspending band attaches to the frontal process of the maxilla, the medial palpebral ligament and some fibers also adjoin the frontal belly (F) of the occipitofrontalis muscle. In contrast, laterally, the suspending band attaches to the superficial temporal fascia.
Note: The medial bundle of the malaris muscle is not as well studied as the lateral bundle. Some authors state that it is actually a part of the orbicularis oculi muscle, while other studies describe it as a variation of the orbicularis oculi and suggest naming it the orbitozygomatic muscle. However, there is one common thing in all studies - attachment sites of the medial bundle are similar.
Action
The malaris muscle assists in the skin movement around the lower eyelid and upper cheek. It also participates in providing facial expressions. It is believed that the lateral bundle of the malaris muscle assists the zygomaticus major in raising the angle of the mouth and upper lip during smiling and laughing. At the same time, this portion of the malaris muscle could also cause crow's feet (wrinkles at the lateral corner of the eye) during smiling and laughing. The lateral bundle also contribute to the dimple formation.
Besides all the mentioned, the malaris muscle also supports the soft tissue of the midface under tension and prevents its sagging. In fact, the malaris muscle (its lateral bundle) is believed to be the dynamic missing link between the superficial musculoaponeurotic system of the upper face and the superficial musculoaponeurotic system of the midface, forming a bridge between the superficial temporal fascia and the malar fat pad. Moreover, it makes the superficial musculoaponeurotic system of the midface more muscular than aponeurotic, thus delaying midface aging.
It is essential to mention that the malar fat pad is closely mixed with the skin, and both these structures move as a whole. The skin has a natural tendency to sag with age. However, the malaris muscle reinforces the muscular part of the superficial musculoaponeurotic system of the upper face and midface, acting as a dynamic link and producing a lifting effect on the soft tissue of the cheek. Moreover, there has been no evidence of malaris muscle being found during midface lifting procedures. This indirect proof suggests that people with malaris muscle probably do not need lifting.
With aging, the soft tissue of the face gradually loses volume and elasticity; thus, it tends to descend. The midface aging is characterized by sagging of the malar fat pads, malar bag formation, and laxity of the periorbital skin and the lateral corners of the eyes. The malaris muscle prevents the relaxation of the soft tissue of the midface by helping the orbicularis oculi to retain ligaments. Therefore, it maintains and holds the soft tissue and malar fat pad in place.
Additionally, the malaris muscle contributes to the contour and aesthetic appearance of the midface. There is a strong link between people with prominent cheekbones and malaris muscle - they usually have this muscle. Moreover, the Korean population is known to have the most prominent cheekbones among all Asians, and as described earlier, they are also known as one of the populations that show the highest numbers of malaris muscle. This relationship may also explain their ageless appearance.
The suspending bundle of the malaris is also involved in midface aging (especially in the periorbital region), and it is believed that this bundle sustains the infraorbital structures. Additionally, the palpebromalar groove (a deep groove found on the medial side of the eyes) may be caused by a combination of these two factors - the laxity of the lateral attachment of the suspending bundle and a thin orbicularis oculi muscle. This combination further leads to the protrusion of the infraorbital fat.
While there has not been much research on the medial bundle of the malaris muscle, the existing studies suggest that it could prevent intraorbital fat herniation, as well as it prevents the drooping of the suborbicularis oculi fat pad. Additionally, this bundle might be involved in causing the nasojugal fold.
Innervation
The malaris muscle is innervated by the temporal and zygomatic branches of the facial nerve (CN VII). The lateral band and the lateral aspect of the suspending band receive nerve supply from the temporal branches, while the medial band and the medial aspect of the suspending band are innervated by the zygomatic branches.
References:
- Kampan N, Akita K, Mahakkanukrauh P. The malaris muscle concept reconsidered. Anat Cell Biol. 2019 Jun;52(2):134–139. PMID: 31338229.
- Kampan N, Tsutsumi M, Okuda I, Nasu H, Hur MS, Yamaguchi K, Akita K. The malaris muscle: its morphological significance for sustaining the intraorbital structures. Anat Sci Int. 2018;93:364–371. PMID: 29168108.
- Park JT, Youn KH, Hur MS, Hu KS, Kim HJ, Kim HJ. Malaris muscle, the lateral muscular band of orbicularis oculi muscle. J Craniofac Surg. 2011;22:659–662. PMID: 21415632.
- Zufferey JA. Is the malaris muscle the anti-aging missing link of the midface? Eur J Plast Surg. 2013;36:345–352. PMID: 23700358.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app