- Anatomical terminology
- Skeletal system
- Joints
- Classification of joints
- Joints of skull
- Joints of spine
- Joints of lower limb
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
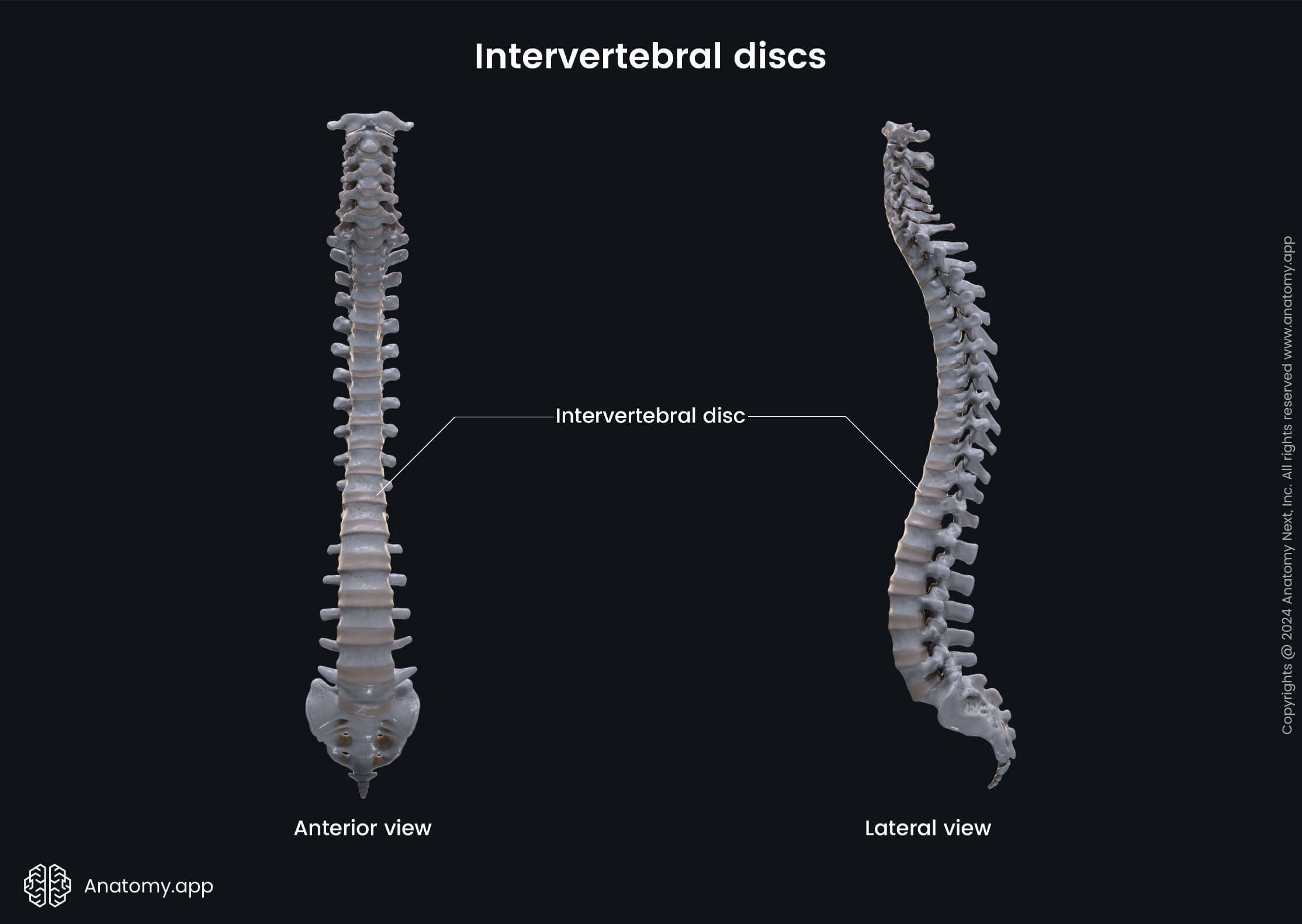
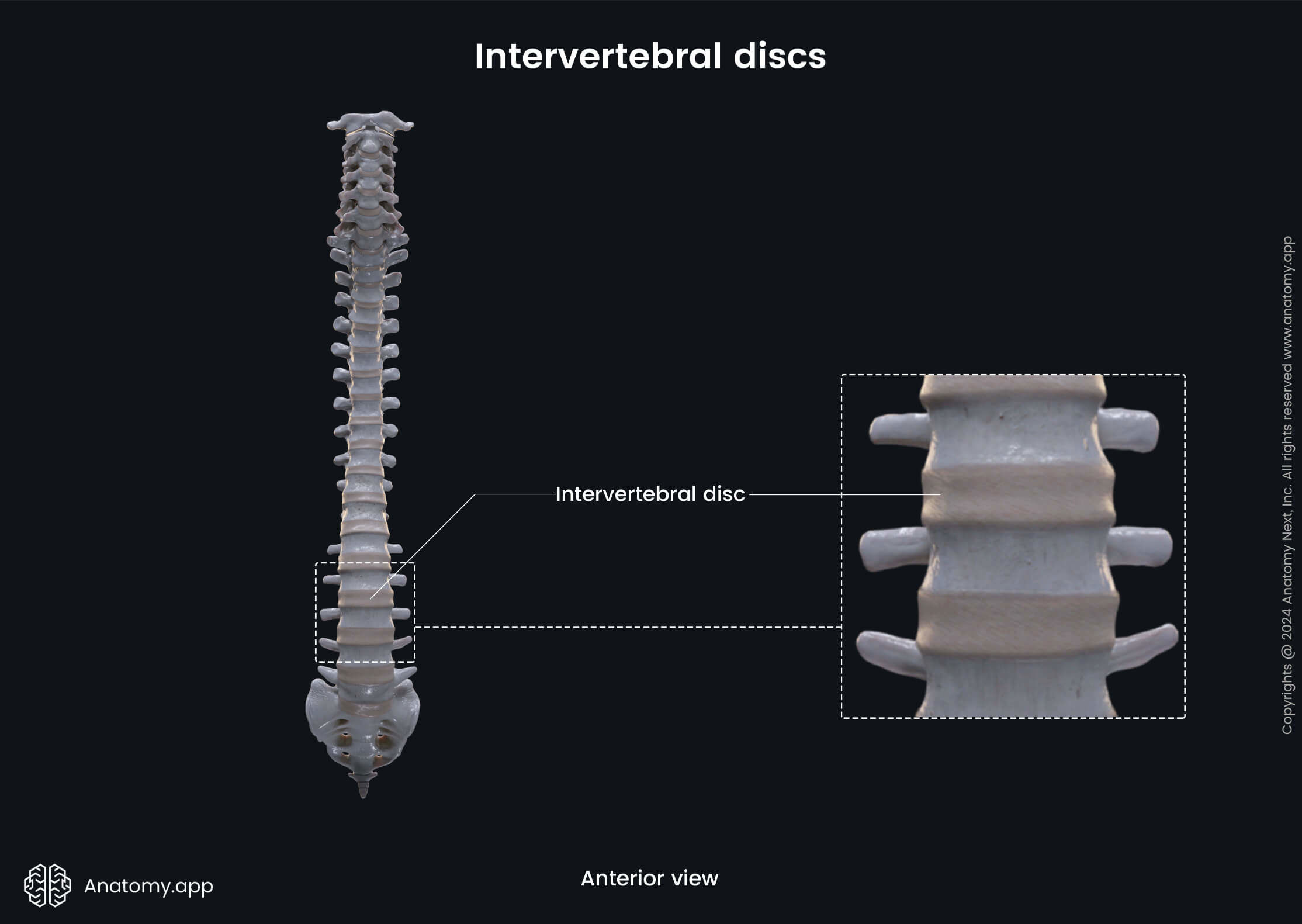
Intervertebral discs
The intervertebral discs (Latin: disci intervertebrales) are complex fibrocartilaginous structures that play a significant part in the biomechanics of the spine. They separate vertebrae from one another and are the main shock-absorbent structures in the spine. The intervertebral discs are found between two adjacent vertebrae starting from the axis (C2) to the sacrum. They are absent in the atlanto-occipital and atlanto-axial joints. Overall, there are 23 intervertebral discs in the spine.
Histologically, the intervertebral discs are secondary cartilaginous joints (also called symphyses). These types of joints have limited mobility. Functionally, the intervertebral discs are classified as amphiarthroses - joints that provide slight movements.
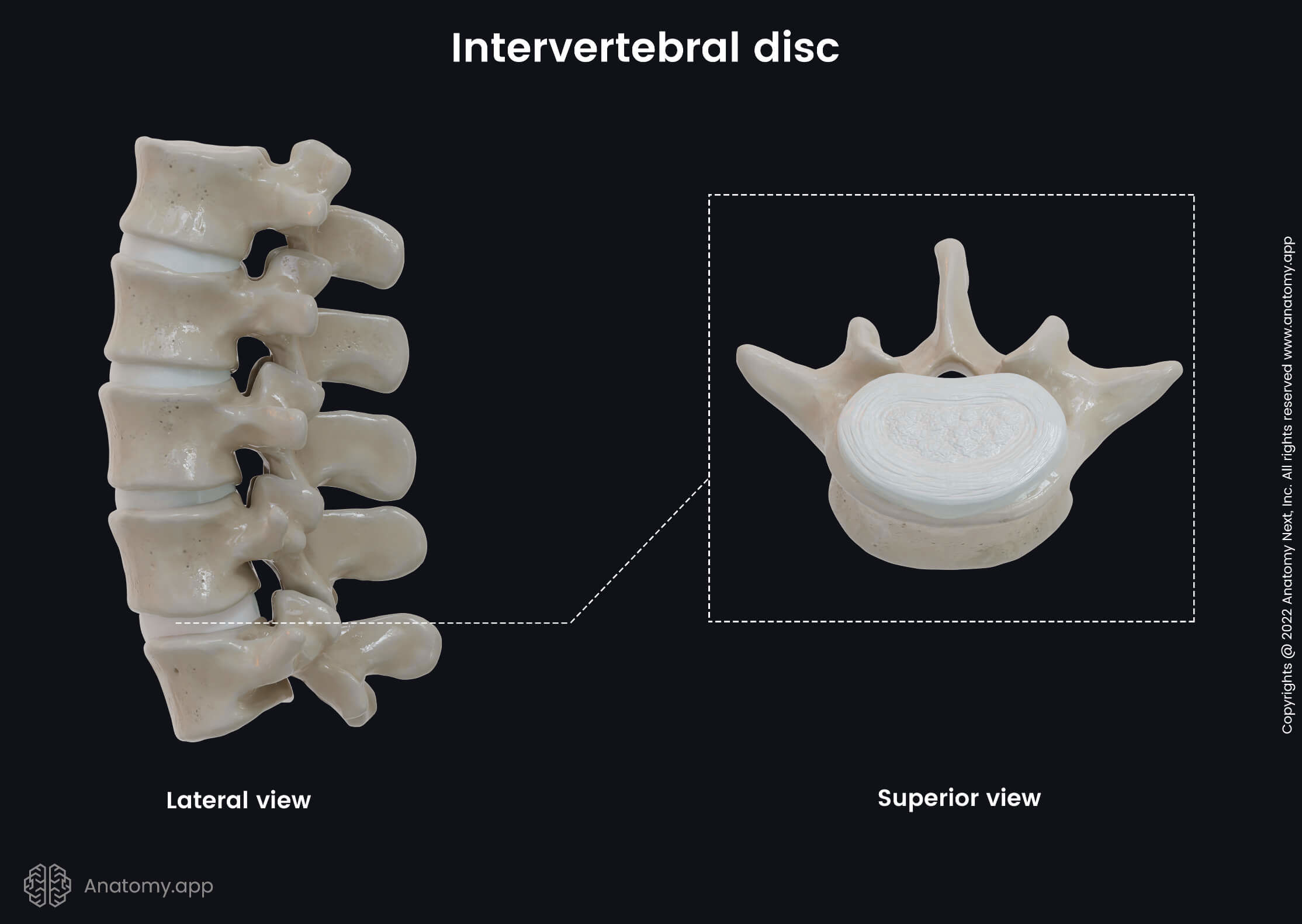
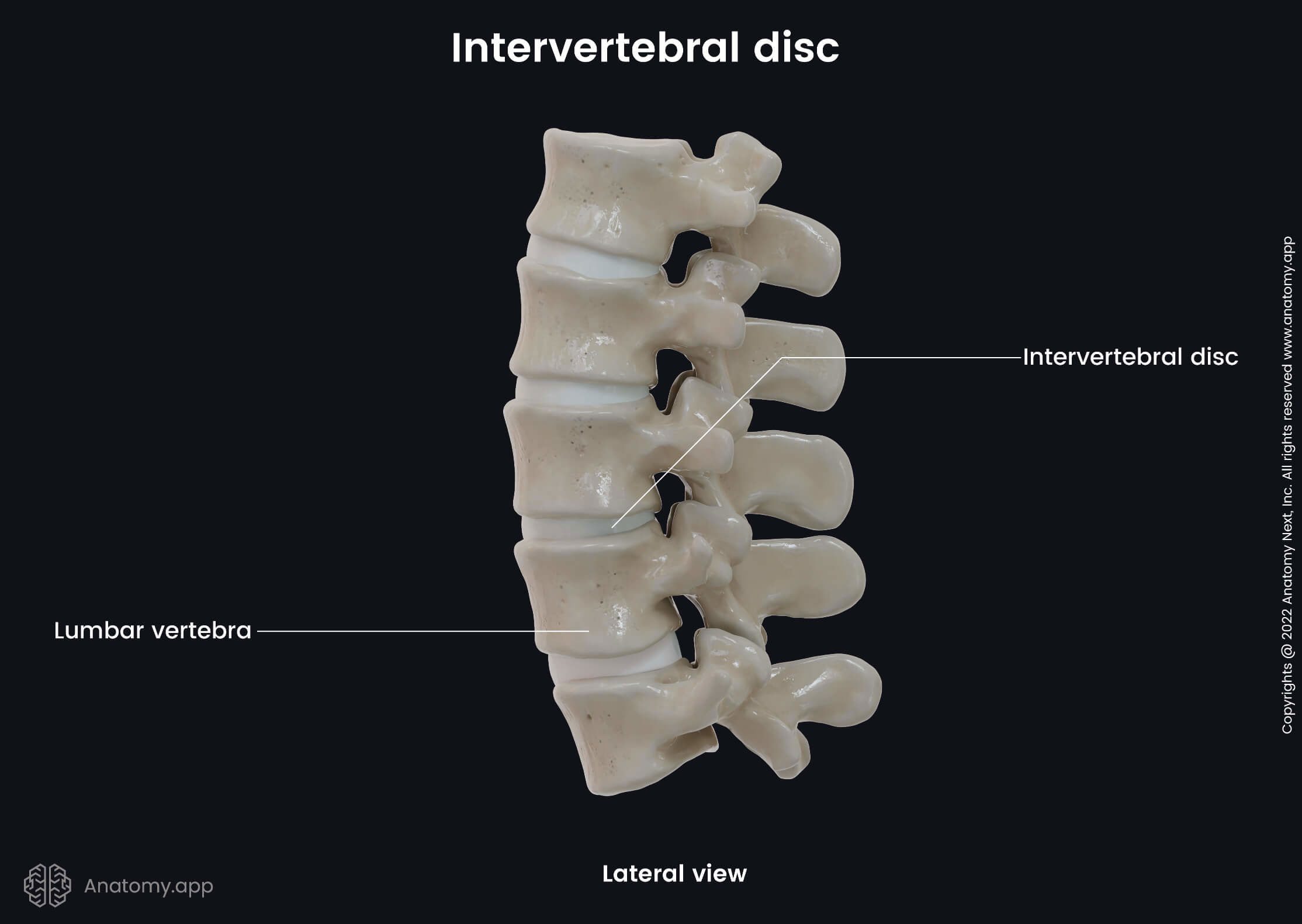
Intervertebral disc anatomy
The thickness of an intervertebral disc varies depending on its location in the spine and within an individual disc. The diameter of a disc usually corresponds to that of the adjacent vertebrae. The thickness of the discs increases towards the sacral part of the spine. Therefore, the intervertebral discs are thinner in the upper cervical spine and thicker in the lumbar region. However, the disc thickness relative to the size of the vertebral bodies is greater in the cervical and lumbar parts of the spine. The intervertebral discs in the lumbar spine are approximately 0.28 - 0.39 inches (7 - 10 mm) thick, and their diameter is 1.57 inches (4 cm).
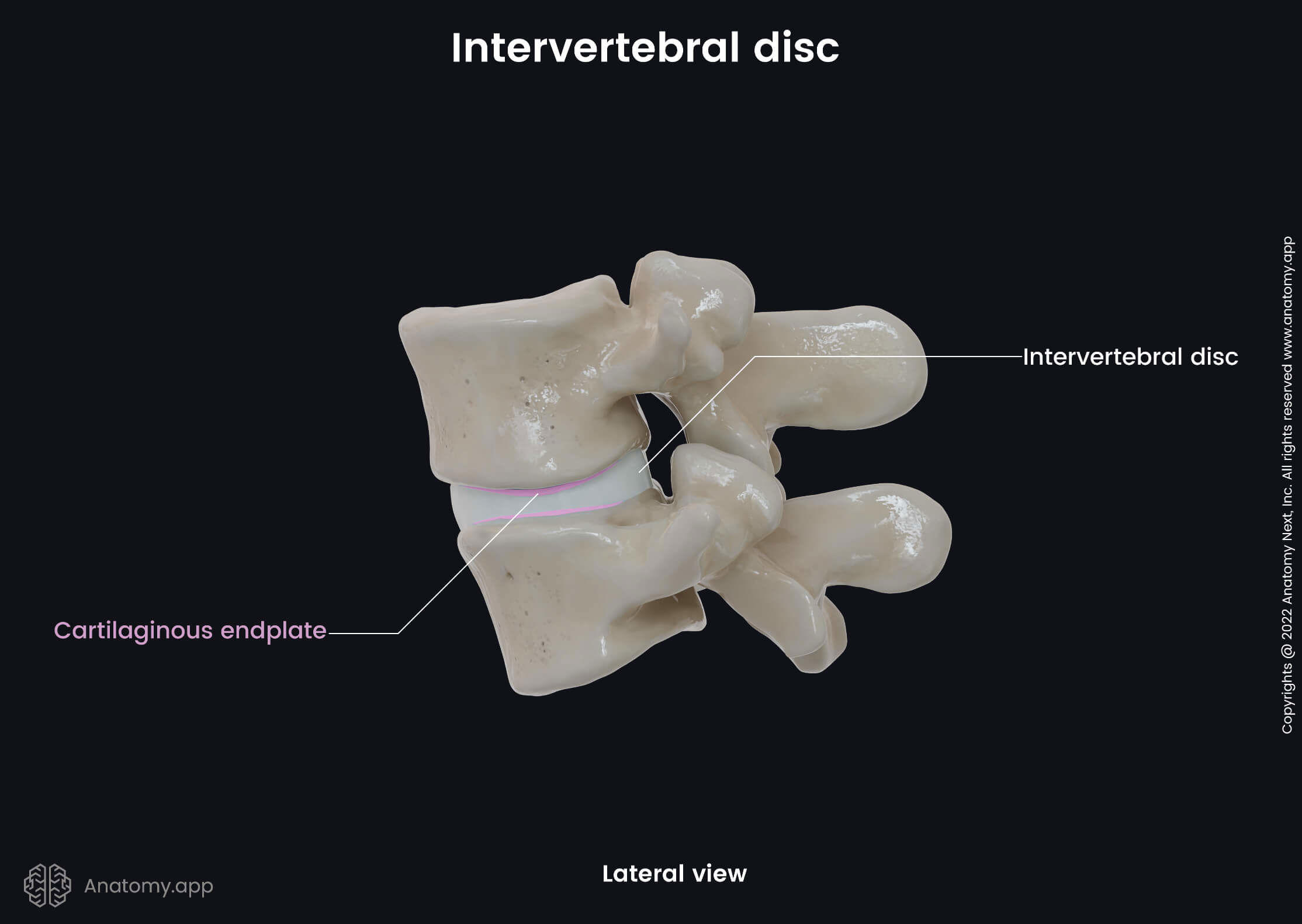
The intervertebral disc resembles a closed water-filled container made up of different types of tissue. The intervertebral discs are composed of three main parts:
- Annulus fibrosus - the outer ring-shaped portion that is made of fibrous connective tissue and surrounds the nucleus pulposus;
- Nucleus pulposus - the inner gel-like core structure;
- Cartilaginous endplate (2) - cartilaginous transition structure at the interface site of the vertebral body and intervertebral disc.
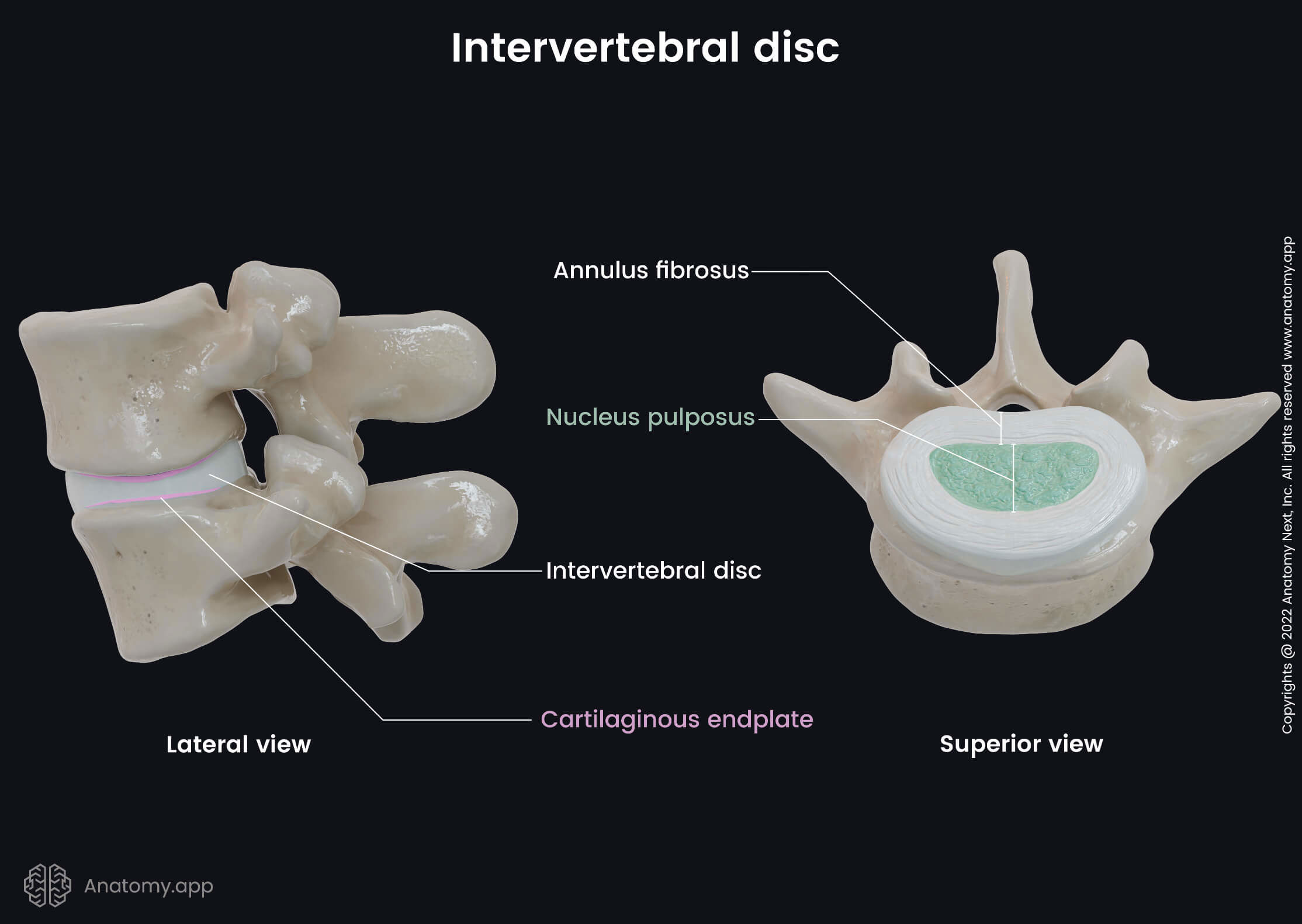
Annulus fibrosus
The annulus fibrosus is the peripheral part of the disc, and it encloses the centrally located nucleus pulposus. The annulus fibrosus is a strong ring-shaped structure containing great amounts of fibroblast cells that constantly synthesize collagen type I and type II fibers. Therefore, the annulus fibrosus is a matrix of collagen fibers that also extend through the cartilaginous endplates and attach to the vertebral bodies.
The collagen fibers within the annulus fibrosus are organized into concentric obliquely, and perpendicular organized lamellar fibers that form a series of 15 - 25 concentric rings called lamellae. The collagen fibers lie parallel to one another within each lamella. These fibers lie at approximately 600 - 650 to the vertical axis between vertebral bodies, alternating to the right and left of it in adjacent lamellae. Adjacent lamellae are interconnected through a bundle of smaller fibers forming the so-called translamellar bridges containing elastin fibers.
The annulus fibrosus can be subdivided into two portions - the outer and inner annulus fibrosus. The inner layer is also known as the transition zone, as next to it is the nucleus pulposus. Cells within the inner annulus are oval-shaped, while they are more elongated within the outer annulus. The inner annulus is not as structured as the inner portion. Also, the outer part contains more significant amounts of collagen fibers.
The structure and orientation of fibers of the annulus fibrosus result in extreme strength and flexibility of the intervertebral discs, allowing them to withstand compressive forces. The annulus fibrosus also supports the nucleus pulposus, and it resists pressure under the load and protects the nucleus pulposus. The annulus fibrosus does not receive any blood vessels or nerves except for its outer part.
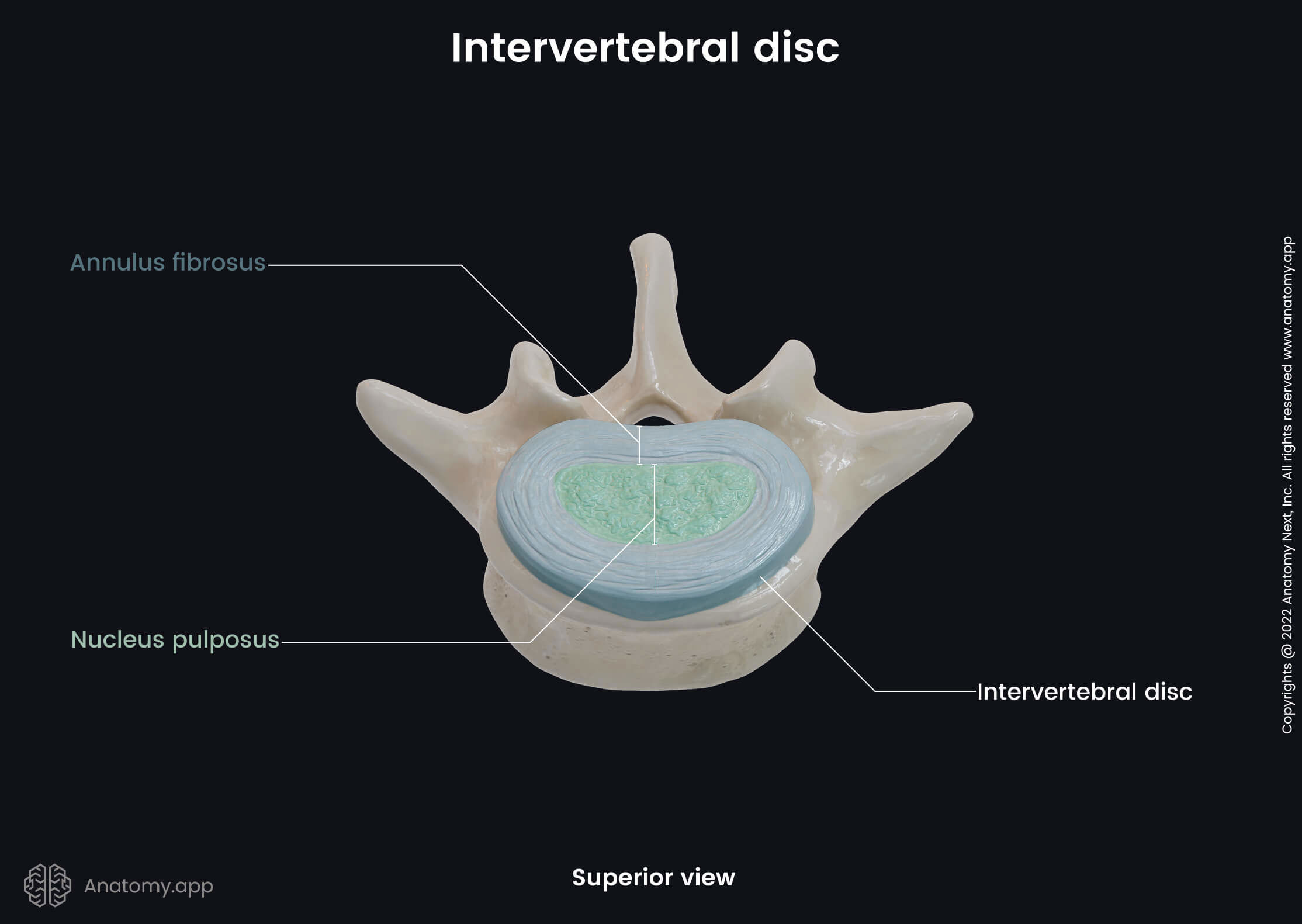
Nucleus pulposus
The nucleus pulposus is located in the center of the intervertebral disc and is the primary shock absorber. The main components of the nucleus pulposus are collagen fibers, elastin fibers, proteoglycans and water. All these components together form a gel-like substance. The water content ranges from 70 to 90 %. It varies throughout the day and gradually decreases with age. In contrast to the annulus fibrosus, the collagen fibers within the nucleus pulposus are randomly orientated, while elastin fibers are radially arranged. Similar to the annulus fibrosus, the nucleus pulposus is also avascular and has no innervation.
Endplates
The endplate is a thin (around 0.04 inches or 1 mm) horizontal-oriented layer of cartilaginous tissue. It serves as a junction site between an intervertebral disc and its neighboring vertebral body. The endplate completely covers the nucleus pulposus, but it does not entirely cover the annulus fibrosus. Every intervertebral disc has two endplates composed of both hyaline cartilage and fibrocartilage.
Hyaline cartilage is more prominent in young adults and neonates and is found toward the vertebral body. In contrast, fibrocartilage is located toward the nucleus pulposus and is more pronounced in older adults. The collagen fibers within the endplates go parallel and horizontal to the vertebral bodies and continue into the disc.
The endplate primarily counteracts the compression forces on the nucleus pulposus and protects it against protrusion and herniation. It also provides nutrient and oxygen diffusion and osmosis from the subchondral bone (bone tissue underneath the cartilage).
Intervertebral disc function
The primary function of the intervertebral disc is to endure a great amount of stress during tension and compression when a person is walking, running or doing any activity that involves the spine. The intervertebral discs are the main shock-absorbing structures, and they all together provide a viscoelastic property. This characteristic allows adjusting to the various loads that the disc has to hold. Therefore, it is a very strong structure that acts as a cushion.
Additionally, the intervertebral discs link and hold together all vertebrae. Therefore, they help to form the spine. Moreover, the intervertebral discs prevent two adjacent vertebrae from grinding and rubbing against each other. Also, they enable movement of the whole spine while at the same time protecting the neural structures.
Neurovascular supply of intervertebral discs
Vascular supply
Almost all parts of the intervertebral disc are avascular and also do not receive nerve supply, except for the outer annulus fibrosus, as there are few blood vessels around the peripheral aspect. These external capillaries branch off the segmental arteries that come from the aorta. Nutrients and oxygen are also received through the endplates from the endplate capillaries that come from the vertebral body.
Venous drainage of the intervertebral discs occurs through the subchondral venous plexus, or venous blood is carried to the veins of the narrow spaces between two adjacent vertebrae.
Innervation
As described previously, the outer annulus fibrosus is the only portion that receives nerve supply. Its posterior aspect is innervated by the branches of the sinuvertebral nerve. The sinuvertebral nerve is a recurrent meningeal branch of the spinal nerve, and it also innervates the posterior longitudinal ligament.
The anterior and lateral parts of the outer annulus are innervated by sympathetic fibers from the gray rami communicantes and nerves derived from the ventral rami of the spinal nerves. These nerves also innervate the anterior longitudinal ligament. Moreover, the outer annulus receives nerve supply from two interconnected nerve plexuses formed within the anterior and posterior longitudinal ligaments.
Intervertebral disc-related disorders
The most common intervertebral disc disorders are related to aging. Intervertebral disc degeneration occurs with age, and it is considered a significant burden on individuals’ quality of life and society due to associated pain. In the younger population, intervertebral disc problems such as disc protrusion and disc herniation are more often related to acute trauma.
Intervertebral disc degeneration
Intervertebral disc degeneration is one of the most common disorders in aging adults causing neck and back pain. Although it usually happens with age, disc degeneration can be initiated by genetic inheritance, obesity, trauma, inflammation or smoking and, therefore, can manifest earlier. The intervertebral discs undergo several structural age-related changes, and some of them include the following:
- The water content of the nucleus pulposus decreases, and the disc loses its height and becomes stiff.
- The nucleus pulposus undergoes fibrosis and presents with clefts and tears that extend into the inner annulus. As the degeneration process continues, they reach the outer annulus.
- The annulus fibrosus also undergoes fibrosis. It loses its characteristic architecture and can start to develop tears and ruptures.
- Like the annulus fibrosus and nucleus pulposus, sclerosis also develops within the endplates, resulting in tears (also called fissures) through which the nucleus pulposus can be pushed out.
Overall, the disc gradually loses its natural structure and can not adequately provide its functions. It becomes stiffer and not so flexible to endure the load. Therefore, disc degeneration becomes a significant cause of back pain, prevalent in the lumbar part of the spine.
Disc protrusion
Disc protrusion (also called a bulging disc) occurs when the entire disc bulges beyond the margins of the vertebrae. During a disc protrusion, the nucleus pulposus breaks through the annulus fibrosus, but the outer annulus remains intact, and the contents of the disc remain whole. This condition usually affects the lumbar spine, and it is most commonly seen at the L4/L5 or L5/S1 vertebral levels. Bulging disc mainly affects men aged between 30 and 55 years.
The causes can be acute due to trauma or weight lifting or chronic due to disc degeneration. It is very common for a disc to compress the adjacent nerve roots on one side or the other upon protrusion. The intervertebral disc protrusion can result in such symptoms as severe pain, spasms, weakness and sensory loss in one of the legs. However, the symptoms of a bulging disc depend on its location in the spine and severity.
Herniated disc
Herniated disc (also called prolapsed disc) is usually associated with the weakness or tears in the annulus fibrosus, due to which the nucleus pulposus extrudes outward through the annulus fibrosus fibers. The nucleus pulposus moves through the disc structures and can spurt out into the vertebral canal or on either side of the disc. It can compress nearby structures such as the adjacent nerve roots located within the vertebral canal, resulting in severe pain, numbness, weakness, tingling and burning sensations.
Any disc can prolapse. However, herniated discs most commonly occur in the lower spine. Therefore, the pain most often presents in the lower back and legs. However, the exact symptoms depend on the affected nerve. Usually, disc protrusion and prolapse are treated with rest, physiotherapy and pain medication. Sometimes surgical treatment may be necessary if neurologic symptoms progress and become worse.
References:
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Magee, D., & Manske, R. (2020b). Orthopedic Physical Assessment, 7e (7th ed.). Saunders.
- Shen, F., Samartzis, D., & Fessler, R. (2014). Textbook of the Cervical Spine (1st ed.). Saunders.
- Waldman, S. (2020). Physical Diagnosis of Pain: An Atlas of Signs and Symptoms (4th ed.). Elsevier.
- Winn, R. (2016). Youmans and Winn Neurological Surgery, 4-Volume Set (Youmans Neurological Surgery) (7th ed.). Elsevier.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app