- Anatomical terminology
- Skeletal system
- Joints
- Classification of joints
- Joints of skull
- Joints of spine
- Joints of lower limb
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
Atlanto-axial joint
The atlanto-axial joint (Latin: articulatio atlanto-axialis) is a complex articulation formed between the first (atlas) and the second (axis) cervical vertebrae. It is composed of three synovial joints: one median atlanto-axial and two lateral atlanto-axial joints.
The atlanto-axial joint is a part of a larger craniovertebral joint group. Craniovertebral joints are articulations between the base of the skull and the first two cervical vertebrae. These articulations include the atlanto-occipital and atlanto-axial joints. They provide a wide range of motion compared to other joints of the axial skeleton.
Atlanto-axial joint | ||
Classification | Synovial pivot and plane-type Diarthrosis | |
Articulating structures | Median atlanto-axial joint | Dens of axis (C2) Osteoligamentous ring (anterior arch of atlas (C1), transverse ligament of atlas) |
Lateral atlanto-axial joint (2) | Inferior articular surface of lateral mass of atlas (C1) Superior articular facet of axis (C2) | |
Ligaments | Anterior longitudinal ligament Yellow ligament Cruciform ligament Tectorial membrane Alar ligaments Apical ligament of dens Accessory atlantoaxial ligament | |
Arterial supply | Deep cervical, vertebral, occipital arteries | |
Venous drainage | Pharyngovertebral veins | |
Lymphatic drainage | Retropharyngeal lymph nodes --> deep cervical (jugular) group of nodes | |
Innervation | 2nd cervical nerve (C1) | |
Movements | Axial rotation (rotation of the head) Very minimal flexion, extension, lateral flexion of the head | |
Classification of atlanto-axial joint
Functionally (depending on the provided movement), the atlanto-axial joint is a diarthrosis. Diarthroses are joints with the broadest range of motion. Histologically (depending on the involved tissue), this articulation is a synovial joint. Synovial joints can be further subdivided according to the type of movements they provide.
The median atlanto-axial joint is a pivot-type joint. It is formed between the odontoid process (dens) of the axis (C2) and the anterior arch of the atlas (C1) together with the transverse atlantal ligament. Pivot-type joints are uniaxial and allow rotational movements. The articulation is formed between the rounded end of one bone (anterior arch of atlas) and another bone (dens of axis) located inside an osteo-ligamentous ring. The median atlanto-axial joint allows the head to rotate from side to side.
The lateral atlanto-axial articulations are classified as plane-type joints. In plane-type joints, the movements are more of a sliding nature. This synovial joint type typically connects flat bones that are similar in size.
Synovial joint characteristics
The atlas and axis are connected via the lateral atlanto-axial joints, and there are no intervertebral discs between them. Also, both vertebrae lack uncinate processes compared to other cervical vertebrae. The articulating surfaces of the atlanto-axial joints are covered by hyaline cartilage. They are enclosed by a joint capsule. Within the capsule, a synovial cavity is located containing synovial fluid. The synovial fluid is produced by the cells of the synovial membrane, and it acts as a lubricant. Ligaments inside and outside the capsule stabilize and strengthen it.
Note: To read more in detail about the types of joints and their functions, please see our article on the classification of joints.
Articulating structures of atlanto-axial joint
The median atlanto-axial joint connects the odontoid process of the axis (C2) called the dens with the osteoligamentous ring. Two structures form this osteoligamentous ring:
- Facet located on the posterior aspect of the anterior atlantal arch (C1)
- Transverse ligament of the atlas situated posterior to the anterior atlantal arch and dens
Each side of the dens has two articulating facets - the anterior and posterior. Each of them contains a separate synovial cavity. The anterior surface of dens (C2) has an oval-shaped facet. It articulates with the facet on the posterior part of the anterior atlantal arch (C1). In contrast, the posterior surface of the dens articulates with the transverse ligament of the atlas.
The lateral atlanto-axial joints are formed between the inferior articular surfaces of the lateral masses of the atlas (C1) and the superior articular facets of the axis (C2).
Fibrous capsules and ligaments
The articulating surfaces of the atlanto-axial joint are surrounded by fibrous capsules. All previously mentioned joints are very mobile, and fibrous capsules are quite loose and thin. Therefore the joints are primarily stabilized with ligaments. Each of the lateral joints has an accessory atlantoaxial ligament. Below the joint, it attaches to the body of the axis and above it to the lateral mass of the atlas.
There are various main ligaments that stabilize the atlanto-axial joint complex, mainly the median atlanto-axial joint. These ligaments include the following:
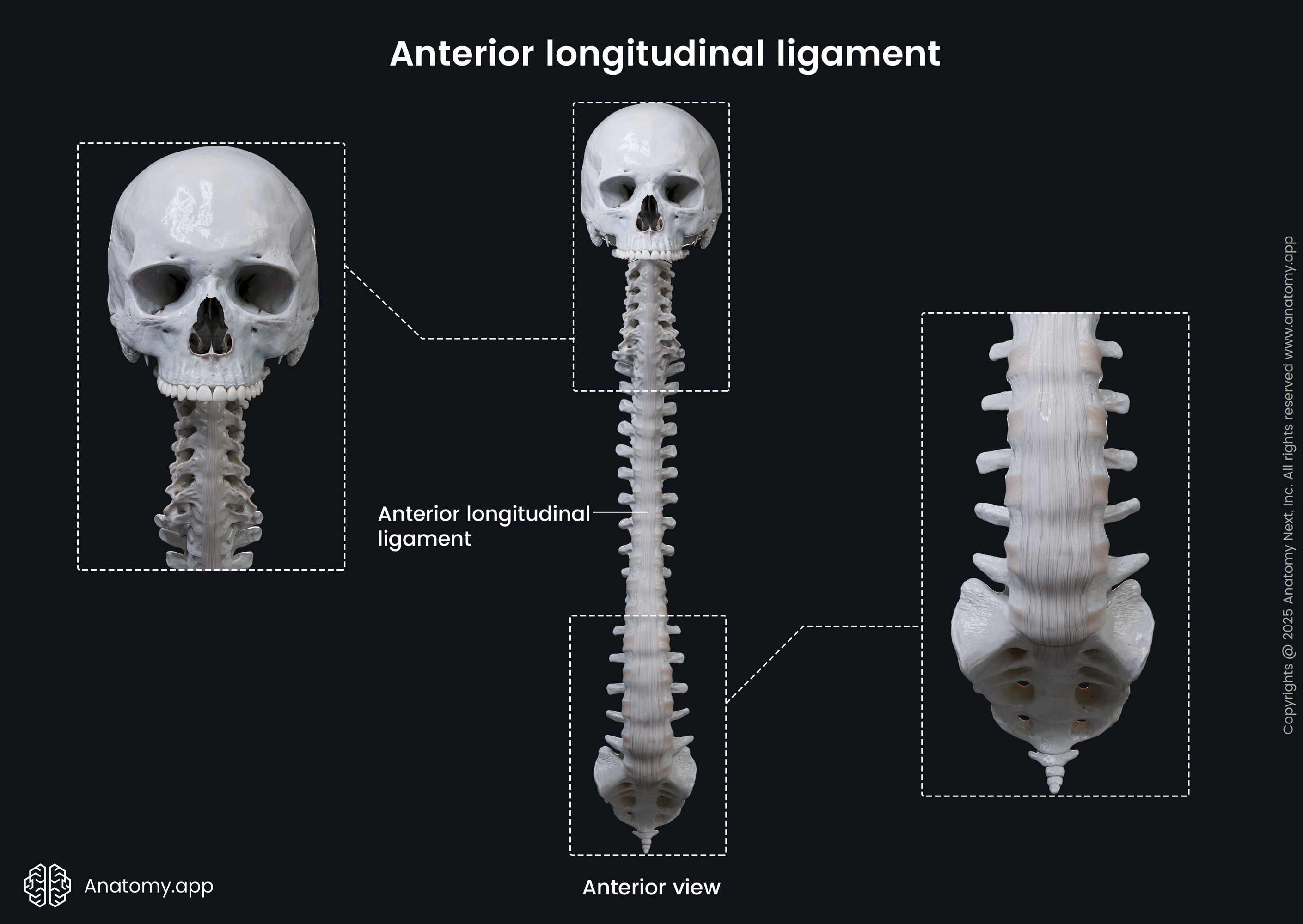
- Anterior longitudinal ligament
- Yellow ligament (ligamentum flavum)
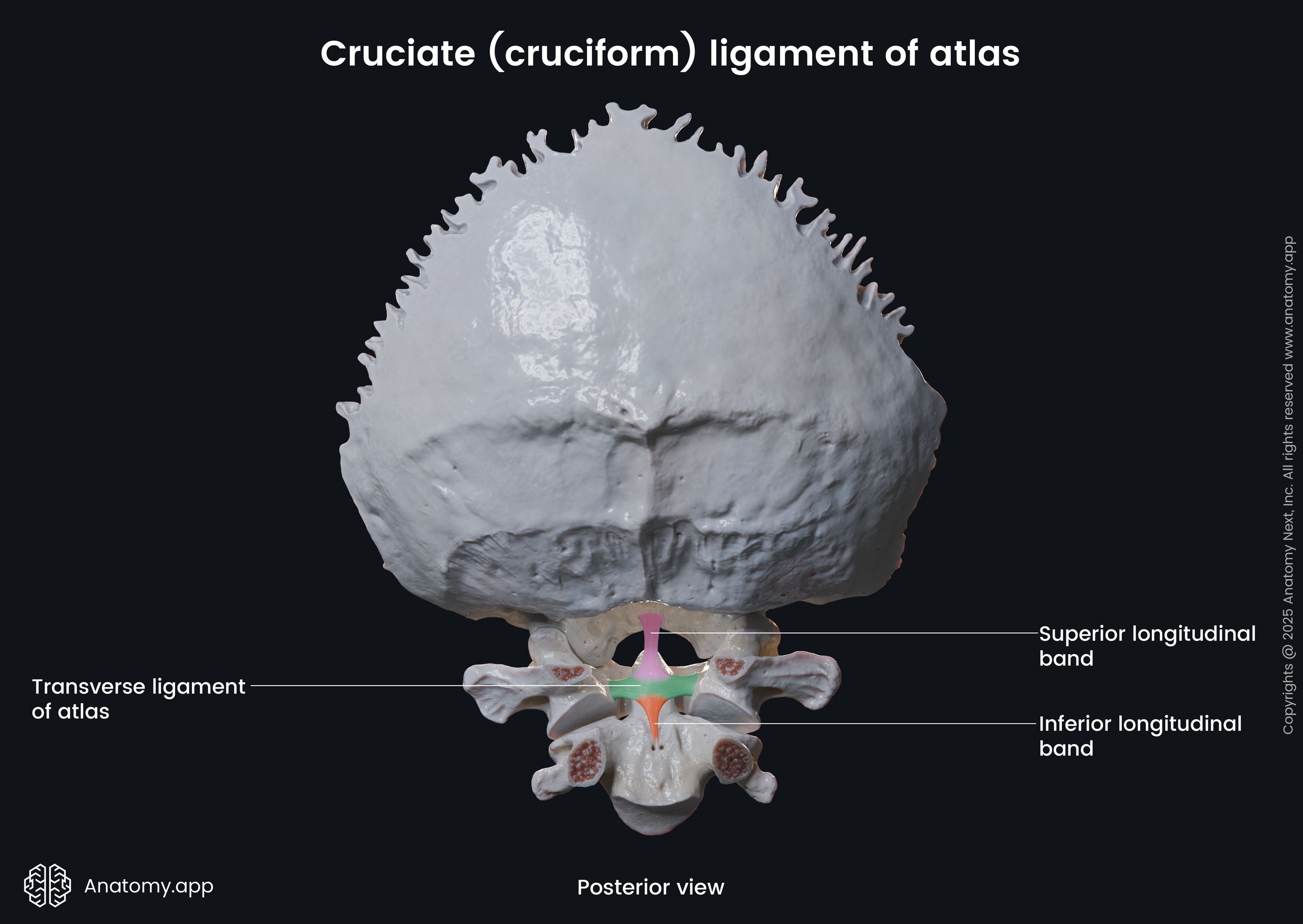
- Cruciform ligament
- Tectorial membrane
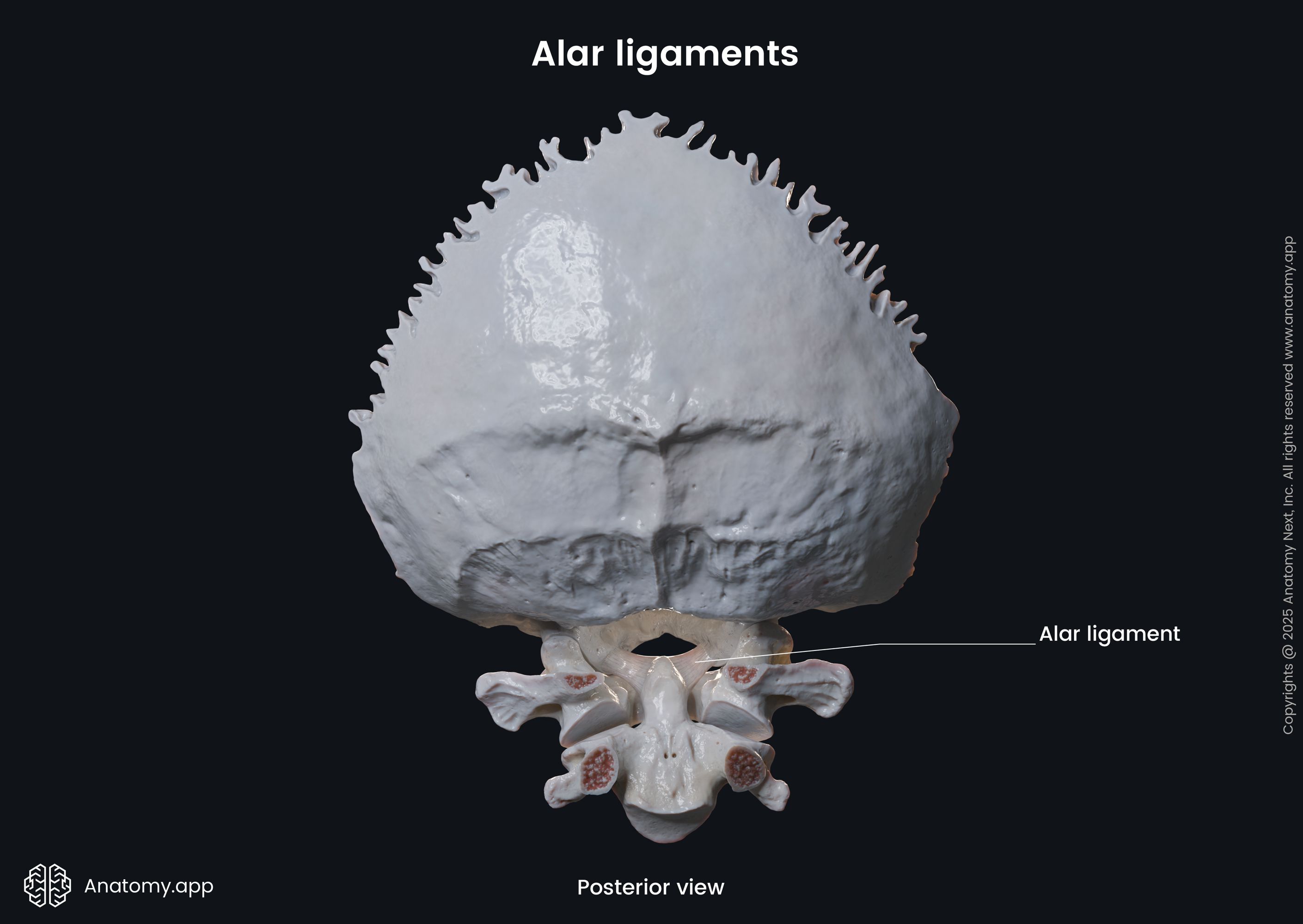
- Alar ligaments
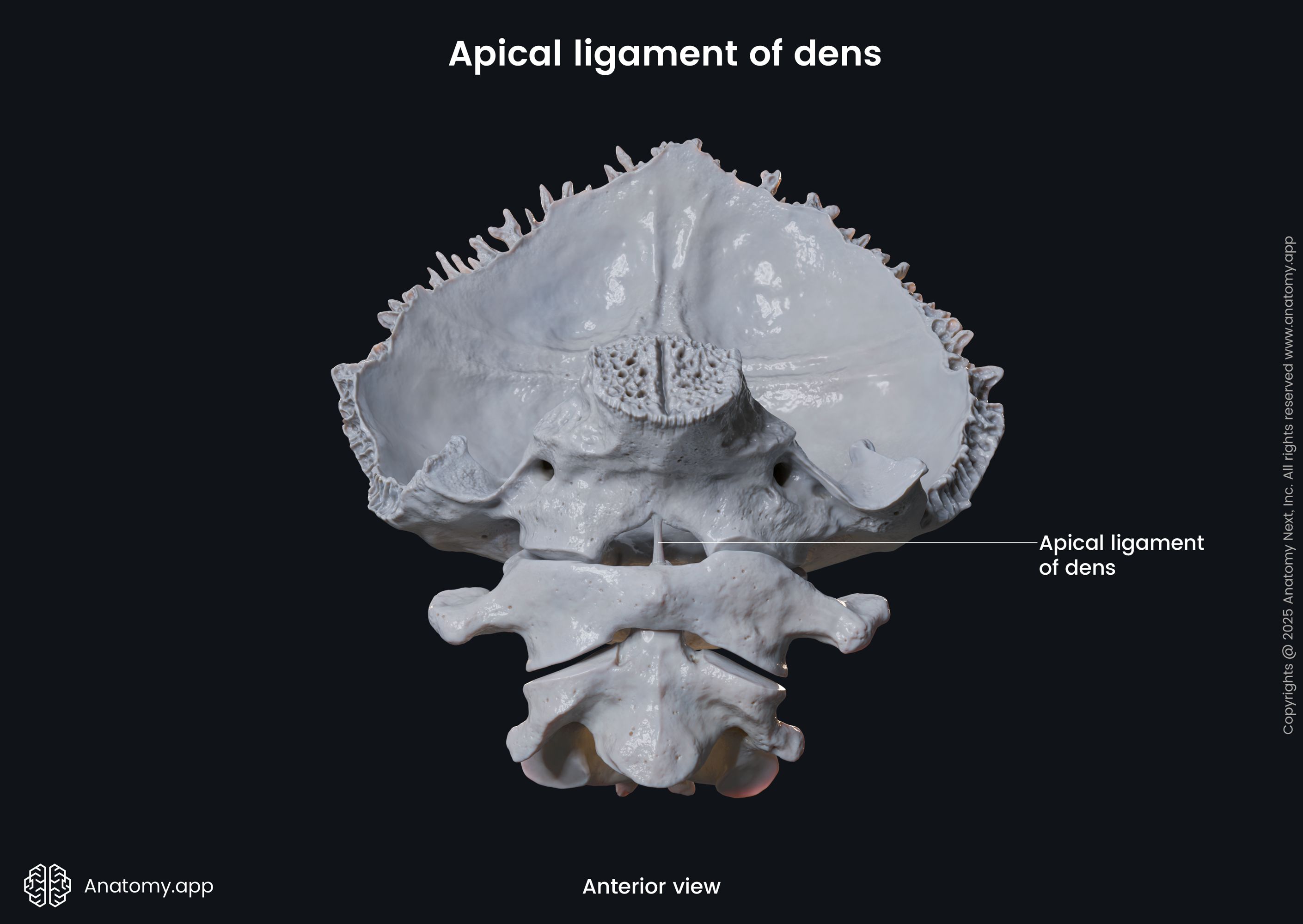
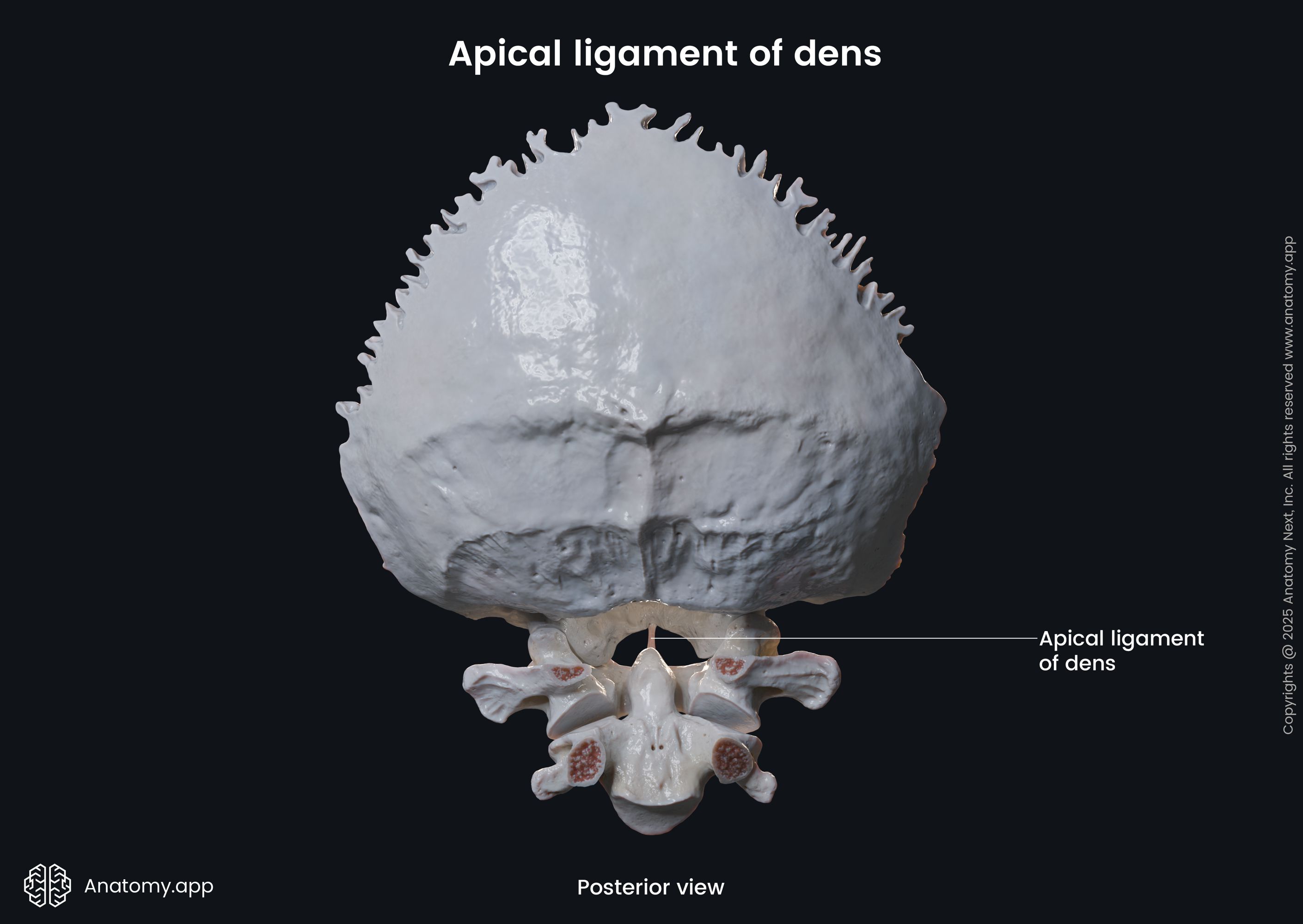
- Apical ligament of dens
The anterior longitudinal ligament connects the basilar part of the occipital bone to the anterior tubercle of the atlas. Then it crosses over the anterior part of the body of the axis and continues further down the vertebral column to reach the pelvic surface of the sacrum.
The posterior parts of the vertebral arches are connected with the yellow ligament (also known as ligamentum flavum). Ligamenta flava (plural) are thick and short bands that link the dorsal parts of adjacent vertebrae in the cervical, thoracic and lumbar spine. In the upper two cervical vertebrae, it connects the inferior border of the posterior atlantal arch with the superior part of the axial laminae.
The primary ligament that contributes to the most strength in stabilizing the occipitoatlantoaxial complex is the cruciform ligament. It is composed of three ligaments that together form a structure shaped as a cross, and these are the transverse ligament of the atlas and two longitudinal bands. The transverse ligament of the atlas is a strong horizontally lying band, and it extends between both tubercles of the atlas located on the medial sides of the lateral masses. The longitudinal bands are known as the superior longitudinal band and inferior longitudinal band. Both are attached to the middle part of the transverse ligament. The superior longitudinal band extends to the basilar part of the occipital bone (clivus). In contrast, the inferior longitudinal band stretches to the body of the C2 vertebra.
Ligaments connecting the axis and occipital bone include the tectorial membrane, paired alar ligaments, apical ligament of dens and longitudinal bands of the cruciform ligament.
The tectorial membrane is the superior continuation of the posterior longitudinal ligament. It has two layers - the superficial layer and deep layer. The superficial layer attaches above the foramen magnum to the clivus of the occipital bone. It further merges with the dura mater of the brain. The deep layer has one median and two lateral parts. The median one reaches the foramen magnum. The lateral ones merge together with the atlanto-occipital joints.
The alar ligaments are a pair of bands connecting the apex of the dens posterolaterally to the medial side of the occipital condyles. The primary function of these ligaments is to limit the atlanto-axial rotation. The apical ligament of dens links the apex of the dens to the anterior margin of the foramen magnum.
Neurovascular supply of atlanto-axial joint
Similar to the atlanto-occipital joint, branches of the deep cervical, vertebral and occipital arteries anastomose with each other and provide arterial blood supply for the atlanto-axial joint. The venous blood drains through the pharyngovertebral veins. The lymphatic drainage occurs via the retropharyngeal lymph nodes, and the lymph is further drained into the deep cervical (jugular) chain of nodes. The innervation is provided by branches of the second cervical spinal nerve (C2).
Movements at atlanto-axial joint
The movement provided by the atlanto-axial articulation takes place in all three joints simultaneously. The main motion is a rotational movement around the axis (C2) - axial rotation. It allows rotating the head from right to left as if looking over the shoulder. This rotation is limited primarily due to alar ligaments. To a minimal degree, flexion, extension and lateral flexion of the head is also possible at the atlanto-axial joint.
Muscles providing atlanto-axial joint motions
Muscles that contribute to the rotational movement of the atlanto-axial joints are the following:
- Obliquus capitis inferior (of the same side - ipsilateral)
- Rectus capitis posterior major (ipsilateral)
- Splenius capitis (ipsilateral)
- Longissimus capitis (ipsilateral)
- Sternocleidomastoid (of the opposite side - contralateral)
- Semispinalis capitis (contralateral)
Muscles providing movements at atlanto-axial joint | |
Rotation (ipsilateral contraction) | Obliquus capitis inferior Rectus capitis posterior major Splenius capitis Longissimus capitis |
Rotation (contralateral contraction) | Sternocleido mastoid Semispinalis capitis |
Note: ipsilateral contraction - the motion (in this case, rotation) happens to the same side as the activated muscle; contralateral contraction - the motion happens to the opposite side.
Related structures
The spinal cord is located posteriorly to the median atlanto-axial joint, and it is the most important “at-risk” neighboring structure (meaning, it can be damaged in case of atlanto-axial joint pathology or trauma). Anteriorly, next to the articulations lies the buccopharyngeal fascia, prevertebral fascia and retropharyngeal space.
Atlanto-axial joint abnormalities
Craniovertebral disorders affect the craniovertebral joint group (includes the atlanto-occipital and atlanto-axial joints), and they are fairly uncommon and usually have poor outcomes. Abnormalities of the atlanto-axial joints can be congenital or acquired. These problems present as a variety of symptoms such as vertigo, tinnitus, hearing loss, hoarseness and difficulty breathing. The main presentation is related to the spinal cord compression at the brainstem or upper cervical level.
Atlanto-axial joint dislocation can occur as a result of transverse ligament injuries. It is sometimes associated with several congenital syndromes, for example, Down’s syndrome. Traumatic rotations can cause atlantoaxial rotatory subluxation. It happens when the force of the rotation is greater than the stabilizing structures of the atlanto-axial joint can bear. It is more common in children. More severe traumas and fractures of the atlas can injure the spinal cord and require surgical treatment.
References:
- Forbes, J., & Das, J. M. (2021). Anatomy, Head and Neck, Atlantoaxial Joint. StatPearls. Published. https://www.ncbi.nlm.nih.gov/books/NBK563271/
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Paulsen, F., Waschke, J., Hombach-Klonisch, S., Klonisch, T., & Peeler, J. (2019). Sobotta Clinical Atlas of Human Anatomy, one volume, English (1st ed.). Urban & Fischer.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app