- Anatomical terminology
- Skeletal system
- Skeleton of trunk
-
Skull
- Neurocranium
- Viscerocranium
- Auditory ossicles
- Sutures of skull
- Topography of skull
- Skeleton of upper limb
- Skeleton of lower limb
- Joints
- Muscles
- Heart
- Blood vessels
- Lymphatic system
- Nervous system
- Respiratory system
- Digestive system
- Urinary system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
Auditory ossicles
The auditory ossicles (also known as ear bones, ossicles; Latin: ossicula auditoria) are three tiny, mobile bones in the middle ear. They are called the malleus, incus and stapes.
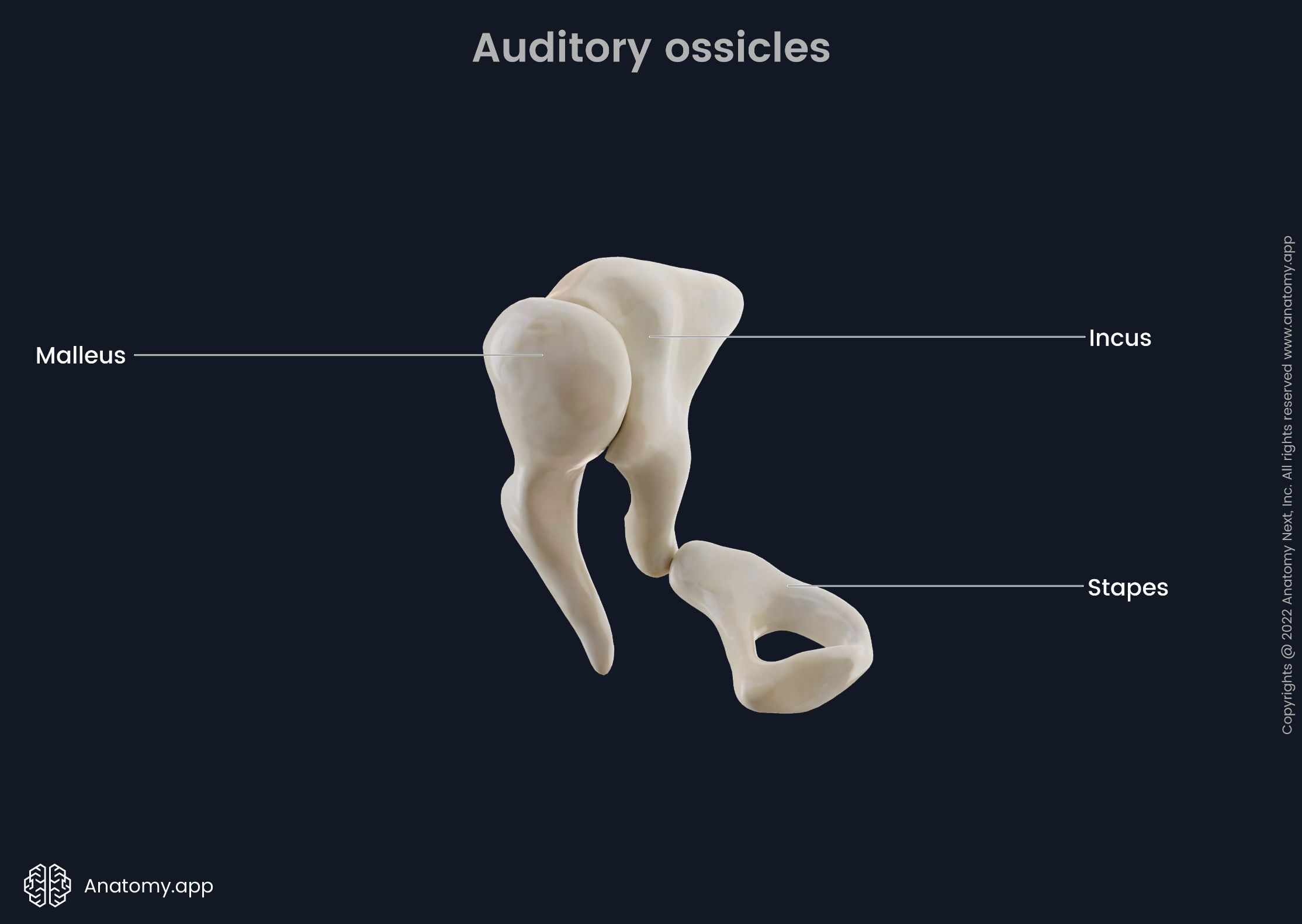
These bones form an ossicular chain that starts from the malleus connected to the tympanic membrane and ending with the stapes at the oval window leading to the internal ear. The incus lies in between the malleus and stapes articulating with both ossicles.
The auditory ossicles, together with the tympanic membrane, transfer and amplify sound waves throughout the tympanic cavity of the middle ear. They convert the sound waves into pressure waves in the endolymph and perilymph of the vestibular canals.
Malleus
The malleus (Latin for “hammer”) is the largest auditory ossicle. It lies next to the tympanic membrane. There are several anatomical parts that can be identified:
- Head of the malleus - the rounded superior part located in the epitympanic recess; the posterior surface of the head articulates with the incus and is, therefore, called the facet for the incus;
- Neck of the malleus - a narrow part of the ossicle below the head;
- Anterior process - located below the neck of the malleus, it is attached to the anterior wall of the middle ear with the help of a ligament;
- Lateral process - also situated below the neck; articulates with the anterior and posterior malleolar folds of the tympanic membrane;
- Handle of the malleus - the part of the malleus below the mentioned processes. It is also attached to the tympanic membrane laterally by connective tissue. A tendon of the tensor tympani muscle attaches to the medial surface of the handle.
Incus
The incus (Latin for “anvil”) is the intermediate bone lying in between the malleus and stapes and articulating with both ossicles. It has three distinct parts - a body and two limbs:
- Body of the incus - the enlarged part of the ossicle located in the epitympanic recess.; its anterior surface articulates with the head of the malleus;
- Long limb - extends parallel with the handle of the malleus; the end of the long limb bends at an angle medially articulating with the head of the stapes;
- Short limb - reaches the upper posterior wall of the middle ear and attaches to it with the help of a ligament.
Stapes
The stapes (Latin for “stirrup” or “saddle”) is the third bone in the ossicular chain, the closest to the internal ear and attached to the oval window - a membrane-covered aperture connecting the middle ear to the cochlea of the internal ear. The stapes is the smallest bone in the human body. It has the following parts:
- Head of the stapes - has a small facet that articulates with the long limb of the incus;
- Neck of the stapes - the narrow part below the head; its posterior surface provides an attachment for the tendon of the stapedius muscle;
- Anterior and posterior limbs - extend from the neck of the stapes and merge with the base; the anterior limb is shorter and thinner than the posterior one;
- Base (or footplate) of the stapes - is attached to the oval window on the labyrinthine wall of the middle ear by a ring of connective tissue fibers known as the annular ligament of the stapes.
Ossicular articulations
All ossicular articulations - joints formed between the auditory ossicles - are synovial. The joint between the malleus and incus (incudomalleolar joint) is saddle-shaped. The joint between the incus and stapes (incudostapedial joint) is a ball-socket type of joint. All articulating surfaces are lined by articular cartilage and the joints are covered by fibrous capsules. The joint cavities are lined by a synovial membrane producing synovial fluid.
Ossicular ligaments
Several ligaments connect auditory ossicles to the walls of the tympanic cavity. Some of them contain collagen fibers, but some of them are just mucosal folds containing neurovascular structures. Three ligaments attach to the malleus; one ligament attaches to the incus and one to the stapedius. The ossicular ligaments are as follows:
- Anterior ligament of the malleus
- Lateral ligament of the malleus
- Superior ligament of the malleus
- Posterior ligament of the incus
- Superior ligament of the incus
- Annular ligament of the stapes
The anterior ligament of the malleus attaches to the neck of the malleus and connects it to the anterior wall of the tympanic cavity. This ligament can sometimes contain muscle fibers called musculus externus mallei (or laxator tympani). The lateral ligament of the malleus attaches to the head of the malleus and extends posteriorly to the tympanic incisure. The superior ligament of the malleus stretches from the head of the malleus to the roof of the epitympanic recess.
The posterior ligament of the incus attaches to its short limb and connects to the fossa incudis. The superior ligament of the incus basically is a mucosal fold connecting the body of the incus to the epitympanic recess. At the base of the stapes lies the annular ligament of the stapes. It is a composition of fibers forming a ring around the base of the stapes and attaching it to the oval window. The annular ligament works as a hinge on which the stapes can move when the stapedial muscle contracts.
Muscles associated with auditory ossicles
There are two muscles associated with the auditory ossicles - stapedius and tensor tympani. The stapedius muscle is a small muscle that originates from the pyramidal eminence of the mastoid wall in the middle ear. Its insertion is located at the posterior surface of the neck of the stapes. Contraction of the stapedius muscle pulls the stapes posteriorly. This prevents excessive oscillation in response to loud noises. The stapedius muscle receives innervation from the facial nerve (CN VII) and arterial blood supply from the branches of the posterior auricular, anterior tympanic and middle meningeal arteries.
The tensor tympani muscle is a long muscle located in the bony canal above the auditory tube. It originates from the cartilaginous part of the auditory tube, the greater wing of the sphenoid and from its own bony canal - the semicanal for tensor tympani in the petrous part of the temporal bone. The muscle inserts into the upper part of the handle of the malleus. Contraction of the tensor tympani muscle pulls on the handle of the malleus medially, which in turn tenses the tympanic membrane. This allows for reducing the force of vibration as a response to loud noises. Tensor tympani is innervated by a branch of the mandibular nerve (CN V3) and receives arterial blood from the superior tympanic branch of the middle meningeal artery.
Movements of auditory ossicles
The malleus moves in accordance with the tympanic membrane. When the tympanic membrane moves inwards or medially, the handle of the malleus follows its movements, as does the long limb of the incus. The inward movement of the long limb of the incus pushes the base of the stapes towards the labyrinth, and the stapes puts pressure on the oval window causing a wave in the fluid (perilymph) located inside the labyrinth.
When the tympanic membrane moves outwards or laterally, the handle of the malleus also moves outwards. The long limb of the incus follows the malleus laterally. The outward movement of the long limb of the incus pulls the base of the stapes away from the labyrinth. The malleus and incus move and rotate together around an axis that projects from the anterior ligament of the malleus to the short process and posterior ligament of the incus.
All three auditory ossicles act as a bent lever in such a way that the base of the stapes makes rocking movements around the anteroinferior border of the oval window. At this point, the annular ligament is the thickest allowing the most gentle motion possible. The movement in the oval window, in turn, starts the movement of the perilymph located inside the internal ear. The waves of the fluid stimulate receptor cells of the organ of Corti. These cells then transmit the generated electrical impulses to the brain with the help of the vestibulocochlear nerve (CN VIII) fibers.
Auditory ossicle problems
The most common medical problem affecting the auditory ossicles is called otosclerosis. Otosclerosis is a bone disease occuring when the lamellar bone gets replaced by woven bone and becomes thicker. If the new thicker bone appears around the base of the stapes, the ossicle may become immobile. This may lead to conductive hearing loss since a proper passage of sound vibrations is not possible.
There are other rare causes for an immobile and fixed base of the stapes that may result in conductive hearing loss. For example, chronic otitis media (inflammation of the middle ear) may lead to the formation of scar tissue inside the middle ear (a process called tympanosclerosis) that impairs its function. Very rarely the base of the stapes can be fixed already from birth. The main treatment in the cases mentioned above is called stapedectomy. During this surgical procedure, the base of stapes is either removed or perforated.
References:
- Drake, R., Vogl, W., & Mitchell, A. (2019). Gray’s Anatomy for Students: With Student Consult Online Access (4th ed.). Elsevier.
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Torsten, L. (2004) Cranial Osteopathy (Second Edition). Elsevier
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app